A 60 year old male with a past medical history of colon adenocarcinoma presents for left leg swelling after a road trip. He denies fever, chest pain, or shortness of breath. Vital signs are within normal limits. On exam, the left lower extremity is neurovascularly intact with a palpable distal pulse. There is swelling and pitting edema of the left thigh and calf compared to the right. Compartments are soft and there is full range of motion without difficulty. Which of the following is the recommended treatment of his suspected condition?
A: Low molecular weight heparin (LWMH)
B: Rivaroxaban
C: Unfractionated heparin (UFH)
D: Warfarin
Answer: Low molecular weight heparin
This patient is likely experiencing a deep vein thrombosis of his lower extremity given his multiple risk factors and exam findings. Therapeutic anticoagulation should be initiated in the emergency department as the patient follows up outpatient. According to the American Society of Clinical Oncology guidelines, the recommended treatment of venous thromboembolism (VTE) in patients with cancer is LMWH.
Rivaroxaban is a reasonable alternative but is associated with an increased risk of bleeding compared to LMWH. Subcutaneous UFH is not recommended for the outpatient treatment of acute VTE due to unpredictable bioavailability and effect requiring frequent monitoring. Warfarin causes an initial pro-thrombotic phase due to inhibition of protein C that would be potentially harmful in the case of active VTE which is why warfarin is typically co-administered with a secondary anticoagulant until the INR is in the desired therapeutic range for 2 consecutive days.
References:
Key NS, Khorana AA, Kuderer NM, et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol. 2020;38(5):496-520. doi:10.1200/JCO.19.01461
Kline JA. Venous Thromboembolism Including Pulmonary Embolism. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020. Slattery DE, Pollack, Jr CV. Thrombotics and Antithrombotics. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
Treatment of Venous Thromboembolism in Patients with Cancer: Subgroup Analysis of the Matisse Clinical Trials, www.researchgate.net/publication/24261105_Treatment_of_venous_thromboembolism_in_patients_with_cancer_Subgroup_analysis_of_the_Matisse_clinical_trials. Accessed 19 Apr. 2024.
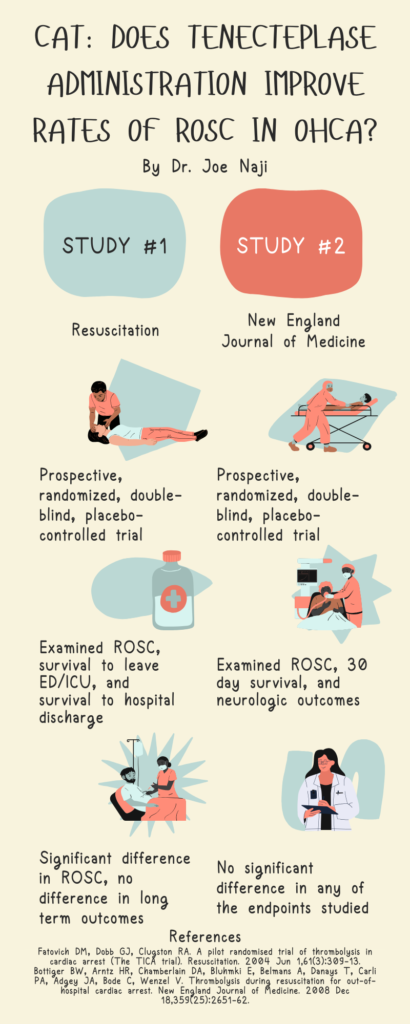
Study 1: A prospective, randomized, unblinded trial of patients in Victoria, Australia, with suspected opioid overdose with RR < 10 and who were unrousable. Exclusion criteria were patients who regained consciousness prior to treatment, those in whom incomplete data was recorded by EMS, and those with response associated with technical errors in recording or administration. Eligibility is not otherwise well-defined in this paper. Requirement for individual patient consent was waived. Subjects were informed of their participation by way of an information letter after regaining consciousness which allowed them to withdraw themselves from the study or seek further information. The objective of the study was to determine the efficacy of IN naloxone compared with IM naloxone for patients with acute respiratory depression secondary to suspected opiate overdose treated in the pre-hospital setting–determined by time to regain RR > 10/min. Secondary outcomes were pts with RR > 10 after 8 mins, proportion with GCS > 11 at 8 mins, proportion requiring rescue naloxone (given as 0.8mg IM dose), and rate of adverse events, defined as agitation, nausea/vomiting, headache, tremor, sweating. 155 subjects (after 27 excluded) were enrolled by paramedics to randomly receive either 2mg IN naloxone by means of a mucosal atomiser (1mg to each nostril) or 2 mg IM naloxone, in addition to BLS. Patients were followed until transport to hospital. Primary outcome of time to regain RR > 10 was 6 min in IM vs 8 min IN condition (P = 0.006). Additionally, a greater proportion of the IM group had regained RR > 10 at 8 mins (P = 0.0163). IN administration resulted in fewer incidents of agitation (P = 0.0278). Other secondary outcomes were not significantly different.
Study 2: Also a prospective, randomized, unblinded trial of patients in Melbourne, Victoria, Australia, with suspected opioid overdose (altered conscious state, pin-point pupils, respiratory rate < 10, unrousable as defined by GCS < 12 and had no major facial trauma, blocked nasal passages or epistaxis). As in the prior study, consent was waived and participation was able to be withdrawn after regaining consciousness. This study’s objective was to determine the effectiveness and safety of concentrated IN naloxone compared to IM naloxone for treatment of suspected opiate overdose in the pre-hospital setting. The primary outcome was the proportion of patients with RR > 9/min and/or GCS > 12 within 10 minutes of naloxone administration. Secondary outcomes included time to adequate response (as defined above), hospitalization, adverse event rate and requirement for ‘rescue’ naloxone (additional 0.8mg IM dose) due to inadequate primary response as judged by the treating paramedics. 172 patients were included in the study (after exclusion of 81 due to not meeting criteria, inadequate training, regaining alertness prior to intervention, and missing equipment) and enrolled by paramedics to receive 2mg IM naloxone or 2mg IN naloxone (concentrated in 1mL and administered 0.5mL per nostril), in addition to BLS. Patients were followed until transport to hospital. Primary outcomes were not significantly different between groups, nor were mean response times, however the number of patients requiring rescue dose naloxone was significantly greater in the IN group vs IM (P = 0.01), even after controlling for age, gender and suspected concomitant alcohol and/or drugs. Other secondary outcomes did not result in significant differences.
Conclusions: In these studies IM naloxone was less likely to result in need for repeat dosing with no significant difference in number of adverse events. In our practice, with patients receiving naloxone in the field and then brought to EMS triage, conditions for monitoring are not always ideal. In those patients in whom opioid overdose is suspected, IM naloxone is less likely to require repeat dosing. Based on my review of the literature, I would preferentially administer IM naloxone in patients with suspected opioid overdose.
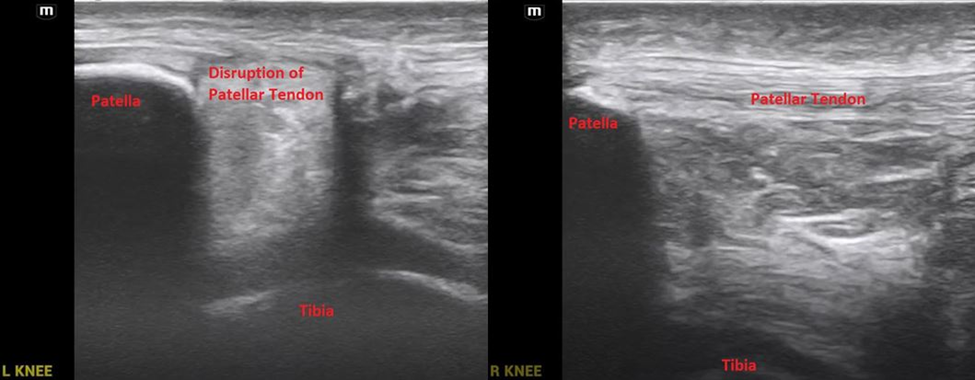
A 20 year old male presents to the emergency department via EMS for left knee pain. He was playing basketball when he jumped and felt a “pop” in his left knee and has been unable to walk on his left leg since. He denies falling. On exam, the left lower extremity is distally neurovascularly intact with normal strength, sensation, and a palpable pulse. There is slight bogginess and swelling with tenderness to palpation to the inferior knee. He is unable to extend at the knee. A point of care ultrasound of the bilateral knees is performed and shown below. What’s the diagnosis?
Answer: Left patellar tendon rupture
Commonly occurs from forced quadriceps contraction or falling on a flexed knee.
Associated with a high-riding patella also known as patella alta which can be appreciated on physical exam and lateral radiographs of the knee.
There is emerging data demonstrating point of care ultrasound as a quick and effective method to diagnose tendon injuries in the emergency department compared to physical exam, x-ray imaging, and MRI.
Treatment:
Incomplete tears with intact extensor mechanism can be immobilized and followed up outpatient with orthopedics.
Complete tears or loss of extensor mechanism should prompt orthopedic consultation in the ED as expedited surgical repair is often indicated.
References:
Bengtzen R. Knee Injuries. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
Berg, K., Peck, J., Boulger, C., & Bahner, D. P. (2013). Patellar tendon rupture: an ultrasound case report. BMJ case reports, 2013, bcr2012008189. https://doi.org/10.1136/bcr-2012-008189
Wu TS, Roque PJ, Green J, et al. Bedside ultrasound evaluation of tendon injuries. Am J Emerg Med. 2012;30(8):1617-1621. doi:10.1016/j.ajem.2011.11.004
A 53-year-old male with a history of chronic daily alcohol use presents to the ED via EMS after a witnessed seizure at home
The medics say he drinks every day, but his last drink was 3 days ago because he was not able to go to the store (history obtained from the sister who witnessed the seizure)
Physical Examination
T 98.3F, BP 177/106, HR 191, RR 22, Sat 93%
Patient appears anxious, uncomfortable, and is actively vomiting blood tinged sputum
He appears confused and is not answering questions appropriately
He is tachycardic and his lungs are clear to auscultation bilaterally
Abd: soft NTND
Differential
Alcohol withdrawal/ Delirium Tremens
Thyrotoxicosis
Sepsis
Pulmonary embolism
Heart failure
Workup and Management
The nurse informs you that the patient is seizing
This patient is exhibiting evidence of delirium tremens (psychomotor agitation and autonomic instability) and alcohol withdrawal seizure
The patient is no longer tolerating his secretions, he is confused, gurgling, and requires a definitive airway
After intubation, you bolus the patient with propofol and start him a propofol infusion
The patient is admitted to the ICU for further management
Teaching Points
ETOH withdrawal begins 6-8 hours after last intake and peaks in 72 hours
Symptom based treatment via the CIWA score can help stratify patients, scores >15 indicate severe withdrawal
Start with IV diazepam at 10mg or lorazepam at 4mg and repeat them in doubling doses
Consider adding phenobarbital for refractory cases (i.e. after 200 mg of diazepam)
Consider propofol as the induction agent and sedative post-intubation as propofol potentiates GABA receptor activity and inhibits NMDA receptors Summary
Delerium tremens can result in death from hyperthermia, arrhythmia and seizures
Sources:
Long D, Long B, Koyfman A. The emergency medicine management of severe alcohol withdrawal. The American Journal of Emergency Medicine. 2017;35(7):1005-1011. doi:10.1016/j.ajem.2017.02.002
Schuckit MA, Author Affiliations From the Department of Psychiatry. Recognition and Management of Withdrawal Delirium (Delirium Tremens): NEJM. New England Journal of Medicine. https://www.nejm.org/doi/10.1056/NEJMra1407298. Published February 5, 2015. Accessed December 9, 2020.
A 43-year-old female with a past medical history of myasthenia gravis presents to the emergency department with shortness of breath. She was just diagnosed with a urinary tract infection and being treated by her PCP with antibiotics. Prior to her developing dyspnea, the patient also mentions experiencing blurry vision and difficulty chewing. She appears in respiratory distress on exam with an SpO2 of 83% on room air. After intubation, what is the most urgent treatment for this patient?
Ceftriaxone with Azithromycin
Methylprednisolone
Physostigmine
Plasma Exchange
Answer is D. Given this patient’s past medical history and symptoms she is most likely in myasthenic crisis, possibly exacerbated by her recent UTI. Ceftriaxone and Azithromycin (A) which could be used to treat community acquired pneumonia would not be helpful in this patient. While corticosteroids (B) are utilized in patients with myasthenic crisis, 60-80 mg of prednisone is usually the corticosteroid of choice, this treatment would not rapidly change the patient’s clinical status. Physostigmine (C.) is an acetylcholinesterase inhibitor often utilized for anticholinergic toxicity. Pyridostigmine is an acetylcholinesterase inhibitor often used as long acting treatment for myasthenia gravis. Treatment for myasthenic crisis includes treating any contributing factors (infection), beginning rapid therapy with plasma exchange or IVIG, and high dose steroids or other immunomodulators. You may want to consider discontinuing acetylcholinesterase inhibitors medications temporarily (as they can increase respiratory secretions) until beginning immunomodulating therapy.
Myasthenia Gravis (no date) REBEL EM – Emergency Medicine Blog. Available at: https://rebelem.com/rebel-review/rebel-review-93-myasthenia-gravis/myasthenia-gravis/ (Accessed: 11 April 2024).
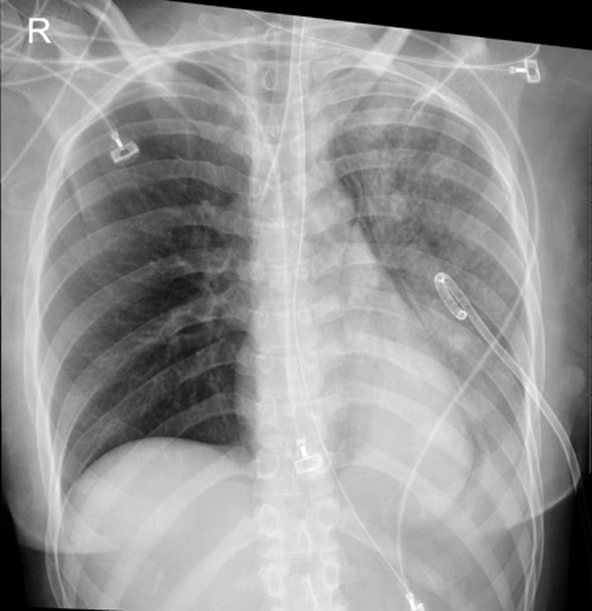
A 40 year old female presents to the emergency department via EMS for shortness of breath. Prior to arrival to the ED, the patient was hypoxic and in severe respiratory distress with absent left lung sounds prompting needle thoracostomy and rapid sequence intubation by EMS. Vital signs are BP 108/70, HR 102, Temp 98F, RR 16, SpO2 99% on 50% FiO2. A left sided chest tube is placed without complication. Chest x-ray confirms appropriate positioning of the endotracheal tube and chest tube with expansion of the left lung. Four hours later, the ventilator is alarming due to elevated peak and plateau pressures. SpO2 is 90%. There is no change with suctioning. A new chest x-ray is obtained and is shown below. What’s the diagnosis?
Answer: Reexpansion pulmonary edema
Reexpansion pulmonary edema is a rare but potentially fatal complication following drainage of a pneumothorax or pleural effusion. The pathophysiology is poorly understood but is thought to involve an inflammatory response leading to increased pulmonary capillary permeability.
Risk factors include large size pneumothorax, large volume pleural effusion, rapid reexpansion, and prolonged duration of symptoms (> 72 hours).
Prevention includes limiting drainage of pleural effusions to a maximum volume of 1.5 liters in one attempt.
Imaging will demonstrate unilateral airspace opacities in portions of the lung that were previously collapsed.
Treatment is supportive with supplemental oxygen and observation. Most patients recover without adverse outcomes.
References:
Nicks BA, Manthey DE. Pneumothorax. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
Asciak R, Bedawi EO, Bhatnagar R, et al British Thoracic Society Clinical Statement on pleural procedures Thorax 2023;78:s43-s68.
Morioka H, Takada K, Matsumoto S, Kojima E, Iwata S, Okachi S. Re-expansion pulmonary edema: evaluation of risk factors in 173 episodes of spontaneous pneumothorax. Respir Investig. 2013;51(1):35-39. doi:10.1016/j.resinv.2012.09.003



")