Case: A 29 year old male with a past medical history of polysubstance use presents to the ED in December via EMS for a suspected overdose. History is limited due to patient cooperation. EMS states that he was found outside in a puddle, minimally responsive. He was given 2mg IM naloxone by EMS and became acutely agitated and combative afterward, requiring 5mg IM midazolam and 5mg IM haloperidol upon arrival. Fingerstick glucose 226. EKG is obtained and shown below.
Exam: BP 182/84, HR 111, T 86.1F, RR 18, SpO2 100%
Disheveled appearing male in wet clothes, intermittently thrashing. Cold to touch. Pupils 5mm bilaterally. No signs of trauma. GCS E3 V2 M5. Moves all extremities equally. Heart rate is tachycardic and irregular.
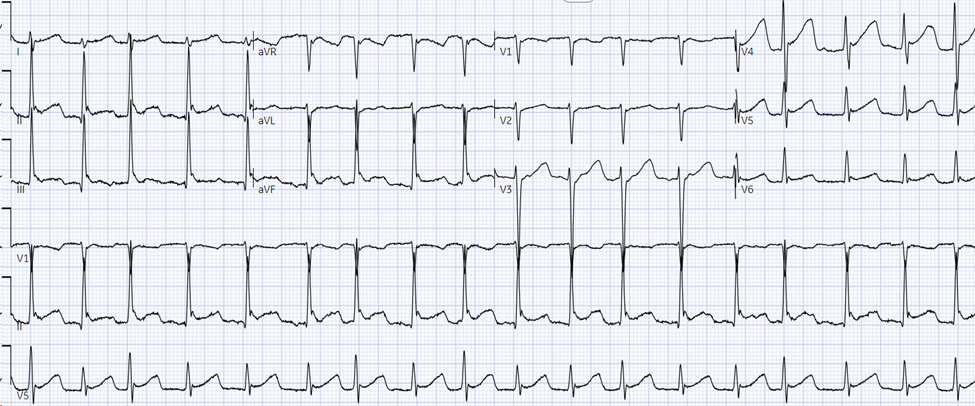
EKG interpretation: atrial fibrillation with rapid ventricular response with Osborn waves
Differential diagnosis: polysubstance use, environmental cold exposure, severe sepsis, hypothyroidism
Case continued: Active rewarming is initiated by removing wet clothes, administering warmed IV fluids, and placing a bair hugger. Labs are notable for a creatinine kinase of 3966. The patient’s temperature, heart rate, and mental status significantly improve within 5 hours, and his repeat EKG shows normal sinus rhythm without Osborn waves. He is ultimately admitted to medicine.
Pearls:
- The cardiovascular response to cold is peripheral vasoconstriction and initial increase in heart rate and blood pressure. As core temperature drops below 32C, there is myocardial irritability and risk of cardiovascular collapse.
- Atrial fibrillation and flutterare common arrhythmias associated with hypothermia.
- Rescue collapse is a term to describe cardiac arrest that occurs during extrication or transport of a profoundly hypothermic patient due to profound myocardial irritability.
- Osborn waves are positive deflections at the end of the QRS complex that are non-specific but may occur in temperatures below 32C.
- Size of the wave correlates with the degree of hypothermia but has no prognostic value.
- As temperature continues to drop, EKG changes are variable but classically include bradycardia with prolonged PR, QRS, and QTc. Heart block or ventricular dysrhythmias may be encountered as well. Asystole is the common final dysrhythmia.
- Rewarming is the treatment of choice.
- Atrial dysrhythmias such as atrial fibrillation will often resolve with warming.
- Cardioversion for unstable arrhythmias should be attempted but may be refractory in severe hypothermia.
References:
Brown DA. Hypothermia. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
Hoek T. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010. 122:5829-5861