A 58-year-old male with past medical history of neurofibromatosis status presents 4 days after emergent neuro IR embolization of a left occipital artery branches after feeling a pop in his surgical site followed by left-sided facial numbness radiating down to the left shoulder with word-finding difficulties. A large, expanding neck hematoma was noted on the left anterior neck. Patient was taken immediately for a CTA to attempt to identify the source of hemorrhage, and upon completion of CT imaging, the patient experienced cardiac arrest. Orotracheal intubation was unsuccessful due to the anatomic distortion from the expanding neck hematoma. Patient underwent emergent surgical cricothyroidotomy and achieved ROSC immediately thereafter.
Surgical Cricothyroidotomy PEARLS:
Indication: can’t intubate, can’t oxygenate, can’t ventilate
- Generally after three attempts failed at orotracheal intubation and unable to maintain oxygenation
- No oral access, masseter spasm, clenched teeth, trismus, structural deformities, laryngospasm, massive hemorrhage, mass effect/displacement of trachea, airway swelling, facial trauma, foreign bodies that cannot be removed from airway safely, no viable connection between upper and lower airway
Equipment: chlorhexidine or povidone iodine solution, 11 blade scalpel, bougie, ET tube
Procedure: The “knife, finger, bougie” technique
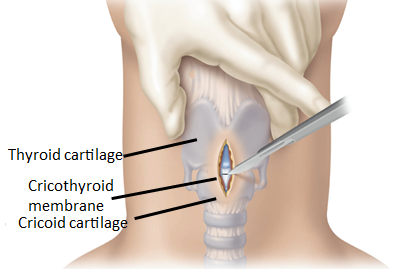
- Palpate the cricothyroid membrane located inferior to the laryngeal prominence (i.e. Adam’s apple)
- Stabilize the larynx using your thumb and middle finger while palpating the membrane with your index finger
- Make a vertical incision along the cricothyroid membrane from the thyroid cartilage to the bottom of the cricoid cartilage. Palpate again with the index finger to confirm the cricothyroid membrane. Make a horizontal stab incision through the cricothyroid memrane and extend the incision 1 cm laterally
- Remove the scalpel and insert the index finger into the trachea. Use your finger as a guide to pass the bougie through the opening. Continue insertion of the bougie until it “hangs up” in the lower pulmonary tract
- Pass the tracheostomy tube or ET tube over the bougie to secure the airway.
References:
Boland C, Nasr NF, Voronov GG. Cricothyroidotomy. In: Reichman EF. eds. Reichman’s Emergency Medicine Procedures, 3e. McGraw Hill; 2018.
Walls R, Murphy M. Manual of Emergency Airway Management. 4th ed. Philadelphia, PA: Lippincott Williams; 2012.
Milner S, Bennett J. Emergency cricothyrotomy. The Journal of Laryngology & Otology. 1991;105(11):883-885.
Holmes J, Panacek E, Sakles J, Brofeldt B. Comparison of 2 Cricothyrotomy Techniques: Standard Method Versus Rapid 4-Step Technique. Annals of Emergency Medicine. 1998;32(4):442-446.