A 2 year old with no past medical history presents with severe left leg pain after falling off a trampoline. He is crying and refusing to bear weight or straighten his left leg. The extremity is otherwise neurovascularly intact. An XR of his left lower leg is shown below. What’s the diagnosis and specifically what type of fracture is it?
Answer: Salter-Harris type II fracture of the proximal left tibia
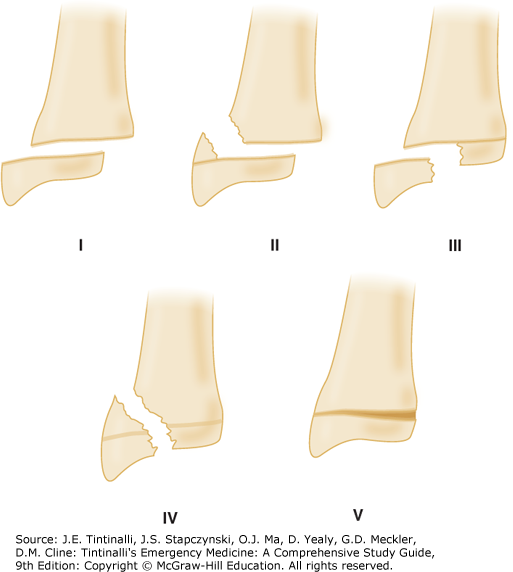
Salter-Harris fractures are fractures of the growth plate, and there are 5 types which are commonly learned with the mnemonic SALTER
Salter Harris Type
Location
Management
1 (Slipped)
Epiphysis separated from metaphysis
Brace, follow up with pediatrician
2 (Above)
Extends though physis and into metaphysis
Splint, NWB, ortho follow up
3 (Lower)
Extends into intra-articular space
Splint, ED ortho consult
4 (Through)
Extends through metaphysis, physis, and epiphysis
Splint, ED ortho consult
5 (ERased)
Physis compression
Splint, ED ortho consult
References:
Mayersak R.J. (2020). Initial evaluation and management of orthopedic injuries. Tintinalli J.E., & Ma O, & Yealy D.M., & Meckler G.D., & Stapczynski J, & Cline D.M., & Thomas S.H.(Eds.), Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw Hill.
A 68 year old male with a history of DM, HTN, and breast cancer presents to the ED with progressively worsening dyspnea over the past three to four days. On exam she is tachycardic to 120, appears tachypneic with accessory muscle usage and pulse ox is 88% on room air. You perform a lung ultrasound which reveals the following:
What is the diagnosis?
Pleural Effusion.
Ultrasonographic findings of pleural effusion:
Fluid appears dark (anechoic) cephalad to the diaphragm and may be homogeneous or heterogeneous depending on the etiology of the fluid.
Lung may be seen as a triangle-like structure floating in the pleural fluid
Thoracic spine sign: the spine is able to be visualized due to loss of mirror artifact as a hyperechoic area posterior to the fluid as the fluid acts a medium through which the ultrasound waves can be transmitted
Case continued:
A pigtail was placed to remove the fluid with the patient experiencing improvement in respiratory status status post drainage of approximately 800mL of fluid.
Resources:
Deschamps, Jade, and Vi Dinh. “Lung Ultrasound Made Easy: Step-By-Step Guide.” Pocus 101, 2023, www.pocus101.com/lung-ultrasound-made-easy-step-by-step-guide/. Accessed 6 Nov. 2024. Co-authors: Jessica Ahn, Satchel Genobaga, Annalise Lang, Victor Lee, Reed Krause, Devin Tooma, and Seth White. Oversight, review, and final edits by Vi Dinh.
Huang, Calvin, Andrew S. Liteplo, and Vicki E. Noble. “Lung and Thorax.” Practical Guide to Emergency Ultrasound, edited by Vicki E. Noble and Bret P. Nelson, 2nd ed., Cambridge University Press, 2011, pp. [specific page numbers if available].
A 51-year-old male with past medical history of HTN, DM presents with right shoulder pain. He states he tripped off the curb and landed on his right shoulder. On exam, there are no palpable deformities, but patient has limited abduction of shoulder and tenderness on palpation of anterior shoulder. An X-ray is obtained and shown below. What’s the diagnosis?
Answer: Acromioclavicular (AC) joint separation
AC joint is composed of the acromion process and clavicle and supported by AC ligament, coracoclavicular ligament
Mechanism of injury is fall directly on shoulder or FOOSH
AC joint injuries range from sprain of ligaments to complete rupture of all supporting ligaments and complete separation of clavicle and acromion
Type I: normal X-ray, due to sprain of ligaments
Type II (X-ray above): widened AC joint, clavicle is displaced <50%, due to rupture of AC ligaments
Type III: clavicle displaced >50%, due to rupture of AC ligaments and coracoclavicular ligaments
Type IV: clavicle is dislocated posteriorly
Type V: clavicle displaced >200% superiorly
Type VI: clavicle dislocated inferiorly
Treatment
Sling immobilization and physical therapy for types I – III
Surgical repair for types IV – VI
References:
Bjoernsen, Lars Petter, and Alexander Ebinger.. “Shoulder and Humerus Injuries.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e Eds. Judith E. Tintinalli, et al. New York, NY: McGraw-Hill, 2016
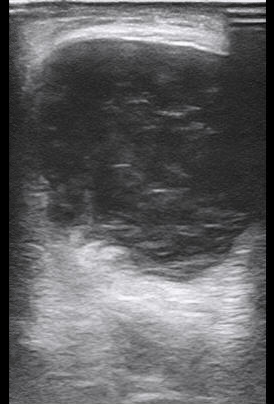
A 5 week old male with no significant PMH and an uncomplicated gestational/birth history presents to the ED after multiple episodes of projectile non-bilious vomiting. Vital signs include a HR of 165, Temp of 98.5F, RR 35, SpO2 100%. Exam is notable for a dry mucous membranes but otherwise is unremarkable. You perform an abdominal ultrasound and find the image below. What is the diagnosis?
Pyloric Stenosis:
– It is caused by hypertrophy of the pylorus leading to gastric outlet obstruction
– Presents with non-bilious projectile vomiting
– Can lead to hyperchloremic, hypokalemic, metabolic alkalosis
– Most commonly presents between 3-6 weeks of age
– Physical exam may reveal an “olive” sized mass in the epigastric region
– Patients may appear dehydrated with protracted disease but generally patients appear well without any signs of peritonitis or even abdominal tenderness
Diagnosis: Ultrasound is the test of choice (97-100% sensitivity and specificity of 99-100%)
– Think Pi: 3.14!
– In the longitudinal view: Length greater than 14mm and pyloric muscle wall thickness greater than 3mm is abnormal.
This patient underwent a pylorotomy without any complications and was successfully discharged.
A 57 yo F with no relative PMH who presented to the ED one day after experiencing a sudden onset, right anterior chest pain after leaning over into her deep freezer. The pain was sudden onset, not relieved with Tylenol, and made it difficult to take a deep breath as well as sleep the night prior. On physical exam, the patient was uncomfortable, with minimal movement She was tachycardic but otherwise vitals wnl. She had tenderness across her right anterior chest at approximately the 6th or 7th rib. A rib series X-ray was suggestive of a minimally displaced acute fracture of the right anterior 7th rib without a pneumothorax. Despite pain medications, the patient remained in debilitating pain and the ultrasound team was called into action!
Serratus Anterior Block:
Anesthetic can be delivered to either of two locations; either the superficial plane between the latissimus dorsi and the serratus anterior muscles; or the deep plan below the serratus anterior muscle, just above the ribs and intercostal muscles. The deep plane is typically preferred as it can deliver anesthetic directly to the rib near the fracture location, thus increasing anesthetic effects. However, it is also more difficult to reach, especially in patients with large habitus, and has higher risk of secondary injury due to closer proximity to the pleural space. To help reduce this risk, the rib can be used as a “backstop” to help prevent the needle from entering pleura. This can be a very effective way to provide pain relief as Figure 1 below demonstrates the target anatomy.
Figure 1
After identifying the location. A needle specific for ultrasound guided nerve blocks with more echogenicity was utilized in plane with the linear probe in a transverse orientation. The needle was slowly advanced with 1cc of Bupivacaine delivered to the skin surface for initial anesthetic before advancing the needle into deeper layers. Hydro-dissection with saline was done at each plane encountered to verify needle location as well as separate planes for easier viewing and targeting. While the deep plane below the serratus anterior was the original target, the patient’s habitus and needle length was unable to reach the deep plane. Therefore, the superficial plane between the serratus anterior and latissimus dorsi was visualized. Bupivacaine Liposome (Exparel), which can be expected to give 48-72 hrs of relief, was injected into this plane without complication.
Within 5-10 minutes, the patient began to feel immediate relief of her excruciating pain. When the primary team reassessed her shortly thereafter, the patient was almost jumping up and down with relief. She experienced no pain and no dyspnea. On a follow-up phone call 3x days later, the patient continued to endorse being pain-free and was amazed at her remarkable turnaround. This case was a perfect example of the extraordinary benefits that a serratus anterior nerve block can provide.
For a detailed step-by-step video on performing a serratus anterior nerve block please watch the following video:
Resources:
1. Bansidhar BJ, Lagares-Garcia JA, Miller SL. Clinical rib fractures: are follow-up chest X-rays a waste of resources?. Am Surg. 2002;68(5):449-453.
2. Gilbertson J, Pageau P, Ritcey B, et al. Test Characteristics of Chest Ultrasonography for Rib Fractures Following Blunt Chest Trauma: A Systematic Review and Meta-analysis. Ann Emerg Med. 2022;79(6):529-539. doi:10.1016/j.annemergmed.2022.02.006
3. Serra, S., Santonastaso, D.P., Romano, G. et al. Efficacy and safety of the serratus anterior plane block (SAP block) for pain management in patients with multiple rib fractures in the emergency department: a retrospective study. Eur J Trauma Emerg Surg(2024). https://doi.org/10.1007/s00068-024-02597-6
Rib fractures can be an incredibly painful condition for patients that is not only painful but also can make breathing difficult and lead to atelectasis and pneumonia. Correct diagnosis of a rib fracture as well as the exact location can help narrow down a differential as well as guide targeted treatments. Diagnosis of fractures can be clinical, but most providers will order imaging. According to the American College of Radiology, in minor blunt trauma that results in only an injury to the ribs, a chest X-ray is rated as “Usually Appropriate” while a rib view radiography is designated a step lower at “May Be Appropriate”. Of note, a rib view radiography is rated as “Usually Appropriate” for any pathologic fractures (i.e Underlying malignancy, metabolic disorders). While useful in identifying secondary injuries such as pneumothorax or flail chest, a chest x-ray can have sensitivities as low as 50% [1]. In the ED CT scans is the standard method through which rib fractures are identified.
A lesser known and utilized diagnostic method is the use of ultrasound, which is becoming more commonly employed in Emergency Departments. While skill level varies and heavily affects results, ultrasound is an effective tool to not only diagnose rib fractures, but also can help deliver a nerve block which provides much needed relief. In fact, in the hands of an experienced provider, ultrasound can be more effective than radiographs; a 2022 meta-analysis of 7 studies with 660 patients demonstrated chest ultrasonography achieving a pooled sensitivity of 89.3% and specificity of 98.4%. [2]
What are we looking for on Ultrasound?
A rib fracture is best visualized in a long view of the rib which would be best classified as a transverse view.
A fracture is best visualized by tracing the outer edge of the rib to visualize any breaks, bulges, or mismatched ends.
The best way to find the fracture: Ask the Patient! Ask them to point to the spot of their worst pain and begin probing there.
Some compression given to the probe may identify buckle fractures as seen in Figure 2 below:
Bansidhar BJ, Lagares-Garcia JA, Miller SL. Clinical rib fractures: are follow-up chest X-rays a waste of resources?. Am Surg. 2002;68(5):449-453.
Gilbertson J, Pageau P, Ritcey B, et al. Test Characteristics of Chest Ultrasonography for Rib Fractures Following Blunt Chest Trauma: A Systematic Review and Meta-analysis. Ann Emerg Med. 2022;79(6):529-539. doi:10.1016/j.annemergmed.2022.02.006
Aortic Dissection can potentially be seen, but identifying a dissection is not the clinical question when performing an US scan of the aorta
Which probe do we use?
Curvilinear Probe
How do we find the aorta and identify its vessels?
Look for the vertebral body as a landmark! The aorta lies above it in the short axis.
“Seagull Sign” – the hepatic and splenic arteries can be seen in the short axis of the proximal aorta in the epigastric region.
Long axis aorta (sagittal plane) – the Superior Mesenteric Artery (SMA) can be seen rising from the aorta in long axis.
“Mantel Clock Sign” – short axis proximal aorta with SMA and splenic vein overlying it superiorly.
Iliac Bifurcation- Trace the lower aorta through its bifurcation into the iliac arteries
What is normal vs. abnormal?
Measure the aorta along it’s course through the abdomen in short axis. > 3 cm from outer edge to outer edge is considered abnormal and concerning for AAA.
Look for dissection flaps and intramural thrombus!
Case: An 80 year old female with a history of COPD presents to the hospital after a fall from standing onto her right side with respiratory distress. She repeatedly states feeling pressure to her face and “my face feels tight”. She appears to be in respiratory distress and is intubated for airway protection. Exam is notable for mild decreased breath sounds BL and for crepitus across her chest, bilateral arms, face, and back. You get a chest X-ray followed which is shown below.
What is the diagnosis? What is the name of the radiologic finding on CXR?
Diagnosis:
The CT and CXR demonstrate bilateral pneumothoraxes with resulting extensive subcutaneous emphysema. In this case bilateral surgical chest tubes were placed with progressive resolution of pneumothoraxes and subcutaneous emphysema.
Ginko leaf sign of the chest. Subcutaneous air tracks along the muscle fibers resulting in a branching pattern that resembles a ginkgo leaf and its branching veins.
A 20 y.o patient presents to the ED after a motor vehicle accident after hitting a ditch. He is fully alert and oriented and is reporting generalized abdominal pain and myalgias. Physical exam is notable for diffuse abdominal tenderness, seatbelt sign with bruising to the right upper chest wall and right flank. VS: HR 70, BP 108/59, RR 18, SpO2 99%
A FAST exam is performed which demonstrates the following:
A CT scan was subsequently performed which confirmed large volume hemoperitoneum with a grade 2 liver laceration.
The patient was subsequently taken to the OR for an exploratory laparotomy. He was ultimately stabilized, and was able to be discharged from the hospital 2 weeks later.
Focused Assessment with Sonography in Trauma: FAST
Focused question: Is there free fluid in the pericardium or abdomen?
Views: Right Upper quadrant, left upper quadrant, subxiphoid cardiac view, pelvic view
Sensitivity of 74% for detection of intra-abdominal fluid
Specificity of 98% for detection of intra-abdominal fluid
Resources:
Netherton, Stuart, et al. “Diagnostic accuracy of Efast in the trauma patient: A systematic review and meta-analysis.” CJEM, vol. 21, no. 6, 18 July 2019, pp. 727–738, https://doi.org/10.1017/cem.2019.381.
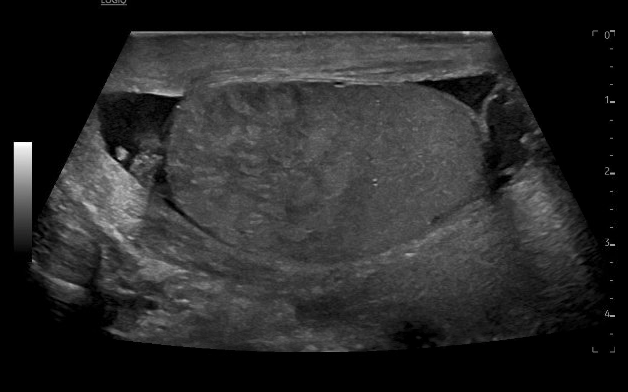
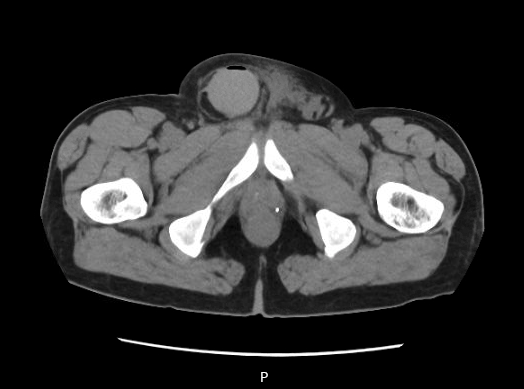
65 year old M presents with significant swelling, discoloration and pain to the right scrotum and penis after inguinal hernia repair 2 days prior. On exam, patient with ecchymosis and erythema of the right testicle and shaft of the penis. There is significant swelling in the inguinal canal, which is not compressible or reducible. You take the ultrasound to bedside to see:
What is the diagnosis?
Answer: Scrotal hematoma
Differentials for this patient include hematoma, hydrocele, scrotal abscess or infection, failure of mesh causing strangulated or incarcerated hernia.
On imaging, you see mixed echogenic fluid collection with no vascular flow noted. This extends from the right groin into the scrotum, with hypoechogenic fluid tracking around bilateral testicles. This is consistent with a scrotal hematoma. There is no bowel noted, ruling out strangulated or incarcerated hernia. There is no “swirl” sign which would be more consistent with scrotal abscess/infection. The mixed echogenic fluid is most consistent with hematoma rather than hydrocele.
Pearls for the bedside scrotal ultrasound:
Use the linear probe
Place the patient supine, place a towel under the scrotum and drape the patient appropriately
Obtain imaging of the unaffected side first for landmarks and comparison
Compare to the affected side, noting echogenicity and landmarks
Visualize both testicles in the same view
Can utilize doppler to assess for flow in concerns for torsion
Yusuf GT, Sidhu PS. A review of ultrasound imaging in scrotal emergencies. J Ultrasound. 2013 Sep 4;16(4):171-8. doi: 10.1007/s40477-013-0033-x. PMID: 24432171; PMCID: PMC3846954.
CT and radiology ultrasound imaging from case are below: