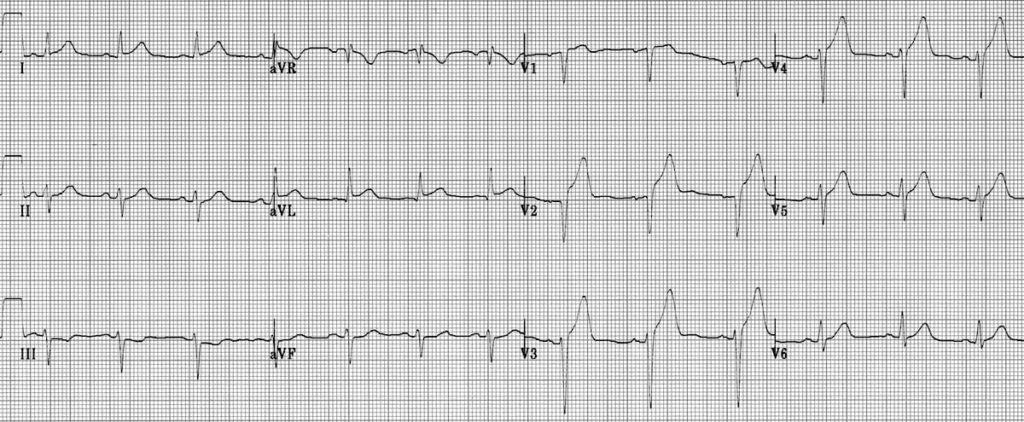
A 68 year old male with a history of hypertension and diabetes presents with chest pain. He was working in his yard when he suddenly felt severe, pressure across his chest. Vital signs are: Temp 98.8, HR 80, BP 162/100, RR 20, SpO2 95% RA. He appears in moderate distress and is diaphoretic. His EKG is shown below. Which of the following is NOT recommended for management of this patient?
A: activation of the cath lab
B: aspirin
C: clopidogrel
D: nasal cannula oxygen
E: nitroglycerin
Answer: nasal cannula oxygen
This patient is experiencing a STEMI. His infarct is likely anteroseptal as evidenced by ST segment elevations and hyperacute T waves in V2-V4 as well as ST segment elevation in I and aVL with reciprocal ST segment depressions in III and aVF. The Air Versus Oxygen In ST-Segment-Elevation MyocarDial Infarction (AVOID) trial conducted in 2015 demonstrated that supplemental oxygen in STEMI patients without hypoxia may increase early myocardial injury and was associated with larger myocardial infarct size at 6 months. Activation of the cath lab and loading with aspirin and clopidogrel are recommended. Nitroglycerin may provide symptomatic relief for this patient but should be used cautiously in patients with evidence of right ventricular infarction.
References:
Stub, D., Smith, K., Bernard, S., Nehme, Z., Stephenson, M., Bray, J. E., Cameron, P., Barger, B., Ellims, A. H., Taylor, A. J., Meredith, I. T., Kaye, D. M., & AVOID Investigators (2015). Air Versus Oxygen in ST-Segment-Elevation Myocardial Infarction. Circulation, 131(24), 2143–2150. https://doi.org/10.1161/CIRCULATIONAHA.114.014494

