52 year old female with a history of breast cancer and recent unilateral mastectomy presents to the ED with the complaint of shortness of breath. Symptoms started earlier this evening and is accompanied by pleuritic, diffuse chest pain, dry cough as well as 4 days of left lateral calf pain. Vital signs include HR 112, RR 30, SpO2 89% on room air, BP 85/61, Temp 99.7F. Physical exam is notable for tachypnea, wheezing throughout all lung fields, and a tender, erythematous left calf. EKG demonstrates sinus tachycardia. A point-of-care cardiac ultrasound is shown below. What’s the most likely diagnosis, and what quantitative ultrasonographic measurement can be obtained to increase your post test probability?

Answer: Massive Pulmonary Embolism; Tricuspid Annular Plane Systolic Excursion (TAPSE)
Primary Use: TAPSE should be incorporated with McConnell sign, D Sign, RV Size and wall thickness and as well as with physical exam / HPI and your pretest probability to determine likelihood of PE. It cannot be used alone to diagnose PE due to the issues listed below.
Steps:
- Obtain a high quality Apical 4 image with clear distinction of the right heart free border
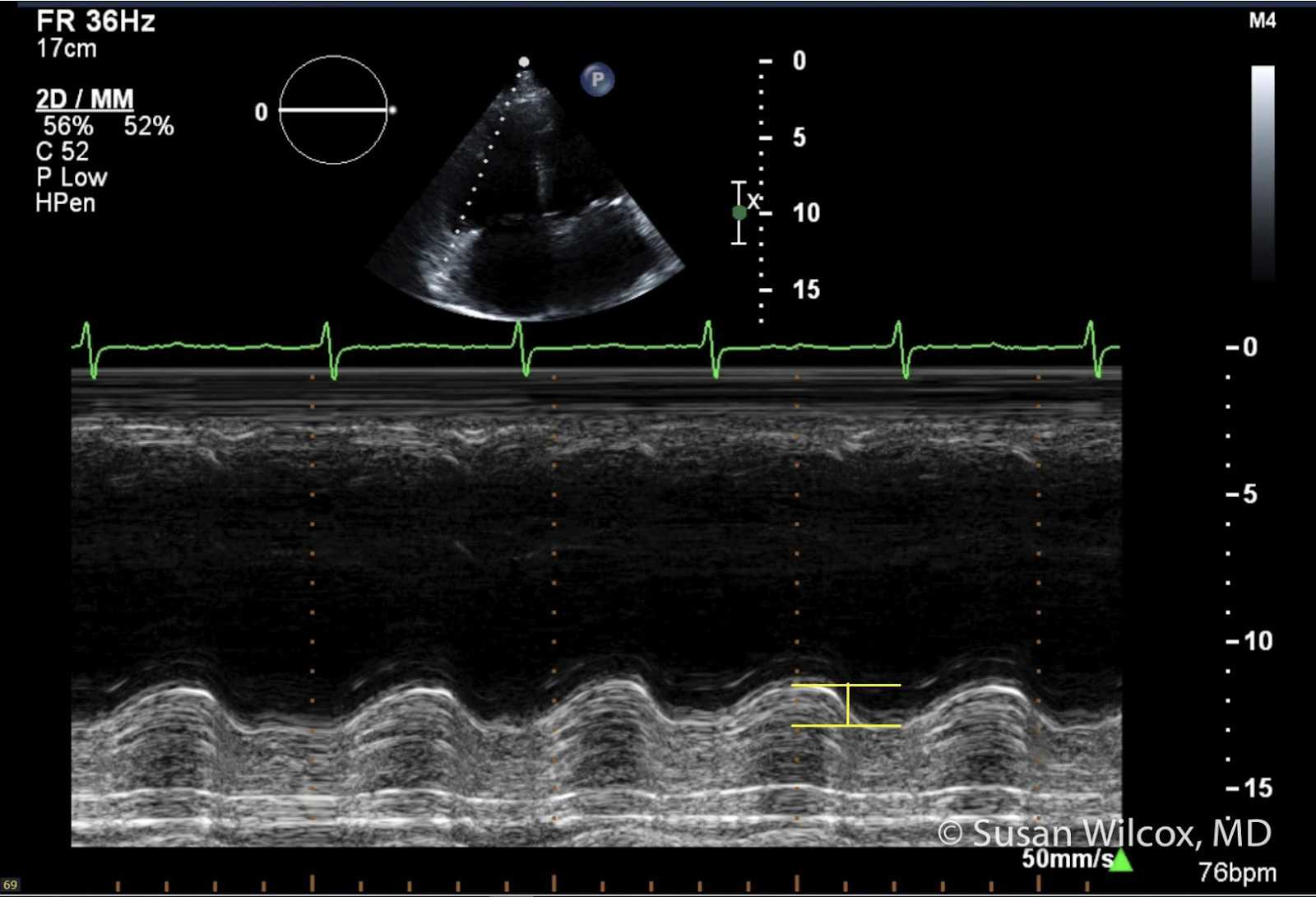
- Enable M mode and measure the right heart free border at TV annulus
- Measure the excursion between nadir and peak of the TV annulus
- Normal > 1.7cm
- Abnormal is < 1.7cm. Individuals with elevated RV afterload will have diminished RV TV movement.
Limitations of TAPSE:
- Overall has a limited sensitivity (53%) and specificity (61%) for PE
- A decreased TAPSE is not specific for PE as other causes of RV strain may have similar findings (Pulmonary HTN, pulmonic stenosis, etc)
- Assesses TV motion in one plane, ignoring the 3D motion of the TV which may be abnormal in individuals with prior cardiac wall motion abnormalities
- Numerical value is adversely affected by improper position of the M mode line
References:
https://www.emrap.org/corependium/search?q=TAPSE#h.sb6k765tgtm2
https://www.thepocusatlas.com/right-ventricular-dysfunction/











