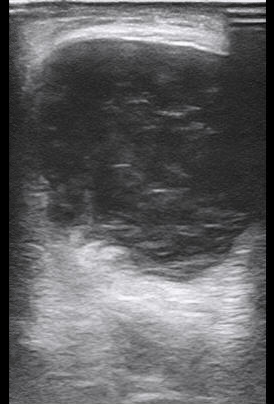
A 5 week old male with no significant PMH and an uncomplicated gestational/birth history presents to the ED after multiple episodes of projectile non-bilious vomiting. Vital signs include a HR of 165, Temp of 98.5F, RR 35, SpO2 100%. Exam is notable for a dry mucous membranes but otherwise is unremarkable. You perform an abdominal ultrasound and find the image below. What is the diagnosis?
Pyloric Stenosis:
– It is caused by hypertrophy of the pylorus leading to gastric outlet obstruction
– Presents with non-bilious projectile vomiting
– Can lead to hyperchloremic, hypokalemic, metabolic alkalosis
– Most commonly presents between 3-6 weeks of age
– Physical exam may reveal an “olive” sized mass in the epigastric region
– Patients may appear dehydrated with protracted disease but generally patients appear well without any signs of peritonitis or even abdominal tenderness
Diagnosis: Ultrasound is the test of choice (97-100% sensitivity and specificity of 99-100%)
– Think Pi: 3.14!
– In the longitudinal view: Length greater than 14mm and pyloric muscle wall thickness greater than 3mm is abnormal.
This patient underwent a pylorotomy without any complications and was successfully discharged.
Aortic Dissection can potentially be seen, but identifying a dissection is not the clinical question when performing an US scan of the aorta
Which probe do we use?
Curvilinear Probe
How do we find the aorta and identify its vessels?
Look for the vertebral body as a landmark! The aorta lies above it in the short axis.
“Seagull Sign” – the hepatic and splenic arteries can be seen in the short axis of the proximal aorta in the epigastric region.
Long axis aorta (sagittal plane) – the Superior Mesenteric Artery (SMA) can be seen rising from the aorta in long axis.
“Mantel Clock Sign” – short axis proximal aorta with SMA and splenic vein overlying it superiorly.
Iliac Bifurcation- Trace the lower aorta through its bifurcation into the iliac arteries
What is normal vs. abnormal?
Measure the aorta along it’s course through the abdomen in short axis. > 3 cm from outer edge to outer edge is considered abnormal and concerning for AAA.
Look for dissection flaps and intramural thrombus!
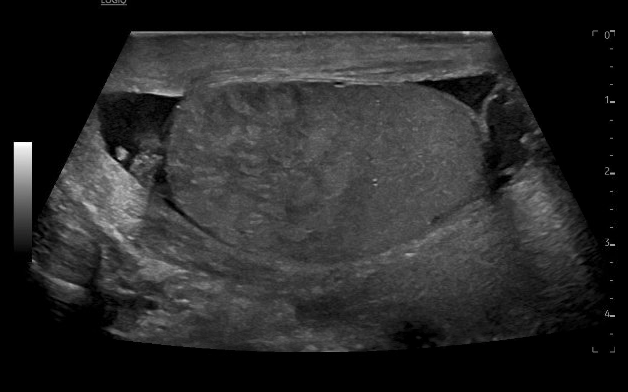
65 year old M presents with significant swelling, discoloration and pain to the right scrotum and penis after inguinal hernia repair 2 days prior. On exam, patient with ecchymosis and erythema of the right testicle and shaft of the penis. There is significant swelling in the inguinal canal, which is not compressible or reducible. You take the ultrasound to bedside to see:
What is the diagnosis?
Answer: Scrotal hematoma
Differentials for this patient include hematoma, hydrocele, scrotal abscess or infection, failure of mesh causing strangulated or incarcerated hernia.
On imaging, you see mixed echogenic fluid collection with no vascular flow noted. This extends from the right groin into the scrotum, with hypoechogenic fluid tracking around bilateral testicles. This is consistent with a scrotal hematoma. There is no bowel noted, ruling out strangulated or incarcerated hernia. There is no “swirl” sign which would be more consistent with scrotal abscess/infection. The mixed echogenic fluid is most consistent with hematoma rather than hydrocele.
Pearls for the bedside scrotal ultrasound:
Use the linear probe
Place the patient supine, place a towel under the scrotum and drape the patient appropriately
Obtain imaging of the unaffected side first for landmarks and comparison
Compare to the affected side, noting echogenicity and landmarks
Visualize both testicles in the same view
Can utilize doppler to assess for flow in concerns for torsion
Yusuf GT, Sidhu PS. A review of ultrasound imaging in scrotal emergencies. J Ultrasound. 2013 Sep 4;16(4):171-8. doi: 10.1007/s40477-013-0033-x. PMID: 24432171; PMCID: PMC3846954.
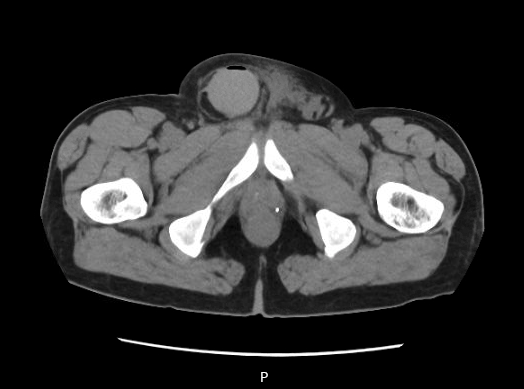
CT and radiology ultrasound imaging from case are below:
Case: 38 y/o female with a history of bilateral renal stones and recent lithotripsy for renal stone who presented with left flank pain and nausea. Symptoms were consistent with previous renal colic symptoms. Following lithotripsy, the patient had resolution of symptoms before flank pain and nausea returned 3 days ago. Vitals BP 142/97, Pulse 93, Temp 98.1 °F (36.7 °C) (Oral), Resp 18, SpO2 99%. The physical exam demonstrated left sided abdominal tenderness and left CVA tenderness. Bedside ultrasound findings below.
Answer: Ureteral stone at the left UPJ with mild-moderate left hydronephrosis
Ultrasound findings in nephrolithiasis
Hyperechoic foci with posterior acoustic shadowing
Location of stone can help predict the probability of spontaneous passage of the stone. Stones in the distal ureter or UPJ are more likely to pass.
Size of stone can help predict the probability of spontaneous passage as well
Hydronephrosis
Greater degree of hydronephrosis reflects more obstruction of ureter and may indicate need for further imaging or procedural intervention
Twinkle Sign
Intense alternating color signal behind calcifications and stones.
Highly suggestive of a kidney stone (sensitivity 99.12%, specificity 90.91%, PPV 99.12%, NPV 90.91%)
Ureteral jets
Representing maintained ureteral flow with color Doppler
Some studies suggest it can predict spontaneous passage of distal ureteral stones
Conclusions:
Ultrasound can be used first-line for imaging to assess for renal stones, though may require follow-up imaging
Ultrasound may prevent repeated radiation exposure with CT in patients with known renal stones
Bedside US can allow for rapid diagnosis and treatment as well as faster discharge when assessing for renal stones
References:
1. Coursey CA, Casalino DD, Remer EM, Arellano RS, Bishoff JT, Dighe M, et al. ACR Appropriateness Criteria® acute onset flank pain–suspicion of stone disease. Ultrasound Q. 2012 Sep. 28 (3):227-33
2. Dillman JR, Kappil M, Weadock WJ, Rubin JM, Platt JF, DiPietro MA, Bude RO. Sonographic twinkling artifact for renal calculus detection: correlation with CT. Radiology. 2011 Jun;259(3):911-6. doi: 10.1148/radiol.11102128. Epub 2011 Apr 1. PMID: 21460031.
4. Gliga, M. L., Chirila, C. N., Podeanu, D. M., Imola, T., Voicu, S. L., Gliga, M. G., & Gliga, P. M. (2017). Twinkle, twinkle little stone: an artifact improves the ultrasound performance! Medical Ultrasonography, 19(3), 272-275. https://doi.org/10.11152/mu-984
3. Ongun S, Teken A, Yılmaz O, Süleyman S. Can Ureteral Jet Flow Measurement Predict Spontaneous Passage of Distal Ureteral Stones? Urol Int. 2018;101(2):156-160. doi: 10.1159/000490498. Epub 2018 Jun 27. PMID: 29949810.
4. Wong C, Teitge B, Ross M, Young P, Robertson HL, Lang E. The Accuracy and Prognostic Value of Point-of-care Ultrasound for Nephrolithiasis in the Emergency Department: A Systematic Review and Meta-analysis. Acad Emerg Med. 2018 Jun;25(6):684-698. doi: 10.1111/acem.13388. Epub 2018 Mar 25. PMID: 29427476.
5. Brisbane W, Bailey MR, Sorensen MD. An overview of kidney stone imaging techniques. Nat Rev Urol. 2016 Nov;13(11):654-662. doi: 10.1038/nrurol.2016.154. Epub 2016 Aug 31. PMID: 27578040; PMCID: PMC5443345.