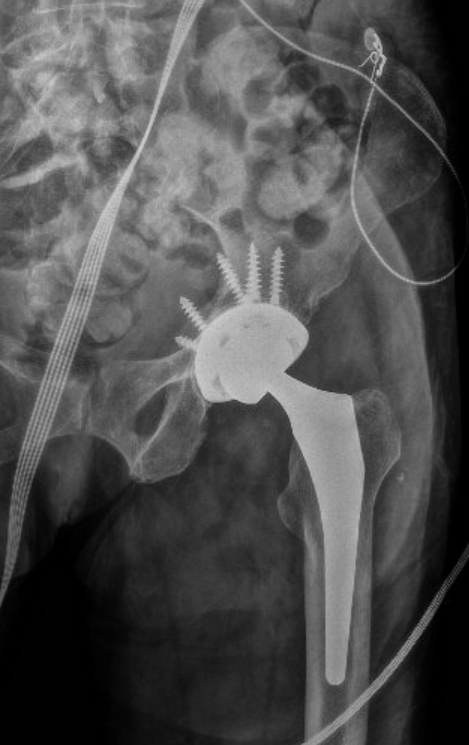
Case: A 60 year old female with a past medical history of a left hip replacement presents with a chief complaint of left hip pain after a fall. Since the fall she has been unable to move her hip and on exam the left leg is visibly shortened, adducted, and internally rotated, otherwise the patient is neurovascularly intact. X-ray reveals the image below. What’s the diagnosis?

Answer: Posterior Hip Dislocation
Case Continued: Under procedural sedation with keto-fol the hip was reduced successfully using the Captain Morgan technique as demonstrated in post-reduction XRs below. The patient was then placed in a knee immobilizer and discharged with an abduction pillow and orthopedic follow up.
- Over 90% of hip dislocations are posterior
- Up to 10% of prosthetic hips undergo dislocation with the vast majority being posterior
- Native hip dislocations are an orthopedic emergency and should be reduced as soon as possible!
- The risk of avascular necrosis increases from <10% to about 25% when reduction is extended from 10 hours to 15 hours
- Prosthetic hip dislocation is not as time sensitive as there is no blood flow to the joint, thus no risk of avascular necrosis.
- Sciatic nerve injury can occur in both native and prosthetic posterior hip dislocations
- There are many different reduction techniques including but not limited to:
- Captain Morgan: https://www.youtube.com/watch?v=lQMWaFX-MeQ
- Whistler technique: https://www.youtube.com/watch?v=Fl71ztyFU7I
- Allis technique: https://www.youtube.com/watch?v=eMVsjwAukU4
- Below is a comprehensive guide to multiple different techniques:
- A CT should be obtained post-reduction of native hips to rule out fractures/loose debris
Resources:
https://www.merckmanuals.com/professional/injuries-poisoning/dislocations/hip-dislocations#v35074190
Tintinalli’s Emergency Medicine Cases A comprehensive Study Guide 9th Edition, Judith Tintinalli