What is cardiac tamponade?
-Cardiac tamponade is a medical or traumatic emergency that occurs when enough fluid accumulates in the pericardial sac to cause compression of the heart, leading to a decrease in cardiac output and obstructive shock.
Risk factors for tamponade:
-Besides hemorrhage (from something such as a stab wound or a left ventricular wall rupture s/p MI), other risk factors include infection (i.e., TB, myocarditis), autoimmune diseases, neoplasms, uremia, inflammatory disorder such as pericarditis.
True or false: the size of the pericardial effusion directly correlates with the risk of developing tamponade.
-FALSE! The rate at which fluid accumulates in the pericardial sac correlates with the risk of developing tamponade. The classic example is a traumatic cardiac injury which leads to hemopericardium. The rapid build-up of blood in the sac quickly leads to the inability of the chambers relax, which leads to decreased venous return, decreased diastolic filling, and decreased cardiac output.
-In situations such as neoplasms where the effusions grow at a much slower rate, there is time for the pericardial sac to stretch; these volumes can be substantially higher without causing tamponade physiology to develop.
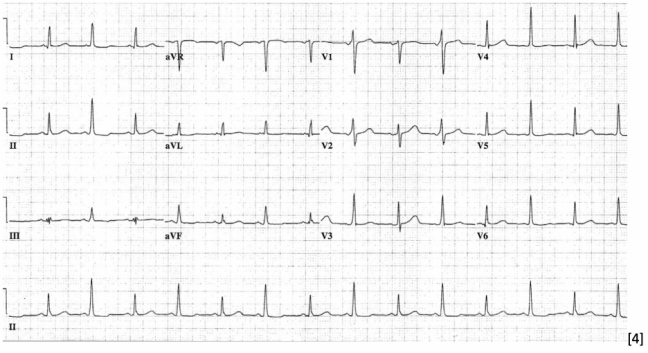
What is one of the first compensatory vital signs seen in tamponade physiology, and also the most common EKG finding?
-Sinus tachycardia. The classic finding of electrical alternans is only present to 5-10% of cases of tamponade.
How does the patient present? What are their physical exam findings?
-Patients present with symptoms consistent with obstructive shock – lethargy, tachypnea, chest pain, palpitations. In severe cases, patients can experience dizziness, syncope, and/or altered mental status.
-Beck’s Triad: hypotension, jugular venous distention, muffled heart sounds.
-Pulsus paradoxus is defined as a decrease in systolic blood pressure of >10mmHg with inspiration. It is an important finding suggesting tamponade but may be absent in people with an elevated diastolic blood pressure, ASD, pulmonary hypertension, or aortic regurgitation.
What are ultrasound findings suggestive of cardiac tamponade?
-A plethoric IVC is the most sensitive finding of tamponade. IVC plethora is defined by a diameter equal or greater to 2 cm with less than 50% collapsibility during inspiration.
-Right ventricular free wall collapse during diastole is considered to be the most specific sonographic finding of tamponade. RV free wall collapse can also be used as a measurement of severity. Initially, collapse of the RV free wall will only be present during expiration, but as the pressure increases, detection is possible throughout the respiratory cycle.
-Right atrial collapse (most often during systole, when the intra-atrial pressure is low) is often observed before right ventricular collapse. RA collapse longer than 1/3 of the total cardiac cycle has been described as an 100% sensitive and specific finding of tamponade.
Sources
Stashko E, Meer JM. Cardiac Tamponade. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431090/
Kalter HH, Schwartz ML. Electrical alternans. NY State J Med. 1948;1:1164-66.
Pérez-Casares, Alejandro et al. “Echocardiographic Evaluation of Pericardial Effusion and Cardiac Tamponade.” Frontiers in pediatrics vol. 5 79. 24 Apr. 2017, doi:10.3389/fped.2017.00079
Mugmon, Marc. “Electrical alternans vs. pseudoelectrical alternans.” Journal of community hospital internal medicine perspectives vol. 2,1 10.3402/jchimp.v2i1.17610. 30 Apr. 2012, doi:10.3402/jchimp.v2i1.17610