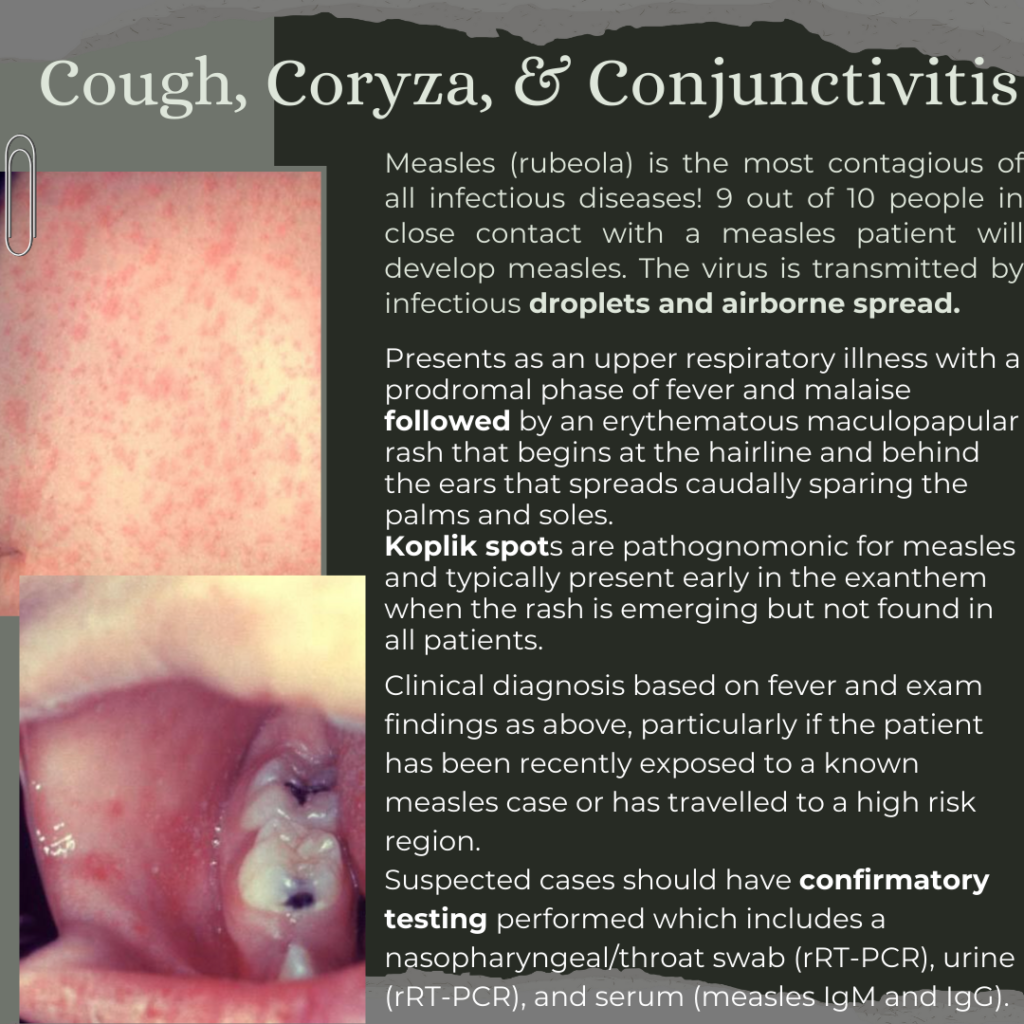
While most cases of measles are mild and will self-resolve, the high infectivity of the virus is a public health hazard due to rare complications of the disease that can cause long-term morbidity and mortality. Particularly high risk populations include unvaccinated individuals, children < 5 years, adults > 20, pregnant women, and immunocompromised patients.
Look forward to part 2 for more details on measles management, treatment, and complications!
Takhar SS, Moran GJ. Serious Viral Infections. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
Nguyen M, Dunn AL. Rashes in Infants and Children. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
1. Shakur H, Elbourne D, Gülmezoglu M, et al. The WOMAN Trial (World Maternal Antifibrinolytic Trial): tranexamic acid for the treatment of postpartum haemorrhage: an international randomised, double blind placebo controlled trial. Trials. 2010;11:40. doi:10.1186/1745-6215-11-40.
2. American College of Obstetricians and Gynecologists (ACOG). Postpartum hemorrhage: ACOG practice bulletin no. 183. Obstet Gynecol. 2017;130:168-186.
Chronic illness, recurrent ulcers in stomach and duodenum most commonly due to H. Pylori and NSAIDs. 10% people in the western world will have this in their lifetime.
Relieved by ingestion of food (usually), milk, antacids (buffers/dilutes gastric acid)
Worsens after gastric emptying, classically the pain awakens patients at night
Chronic ulcers can be asymptomatic or cause painless GI bleeding
NOT (usually) related to PUD: pain after eating, nausea, belching
“Alarm features” for suspicion of cancer –> need more emergent endoscopy: >50 yo, weight loss, persistent vomiting, dysphagia/odynophagia, GIB, abdominal mass, lymphadenopathy, Family hx
Physical Exam: For uncomplicated PUD, expect benign physical exam +/- epigastric tenderness (not sensitive or specific). VS should be normal.
Workup: Generally includes CBC to rule out anemia from chronic GIB. Consider LFT, lipase, EKG, trop, upright CXR, RUQ US to rule out other etiologist that may present similarly with epigastric pain if indicated. Gold standard for diagnosis is endoscopy.
Treatment:
Stop NSAIDs
Proton pump inhibitors: decrease acid secretion from gastric parietal cells, irreversibly bind with H+K+ATPase (proton pump).
Example: omeprazole, pantoprazole.
Heal ulcers faster than any other tx.
H2 receptor antagonists: Inhibit action of histamine on H2 receptor on gastric parietal cells
Example: famotidine, ranitidine.
Dose should be adjusted for patients in renal failure.
Sucralfate: covers ulcer crater, protects it and allows healing, but doesn’t relieve pain as well
Antacids: buffer gastric acid. Use for breakthrough pain. (Ex: Mylanta, Rolaids, Tums, etc)
Dispo: As long as uncomplicated (no bleed, obstruction, perforation, etc), can be discharged from ED with Rx for meds above and referral to PCP or GI.
Gastritis
Not the same as PUD
Acute or chronic inflammation of gastric mucosa (not discrete ulcers)
Causes: ischemia, toxic effects of NSAIDs, steroids, bile, alcohol, H. Pylori, autoimmune processes that destroy gastric parietal cells
Exam: epigastric pain, N/V. Often presents with GIB: hematemesis vs chronic anemia vs melena
References:
Fashner J, Gitu AC. Diagnosis and Treatment of Peptic Ulcer Disease and H. pylori Infection. Am Fam Physician. 2015 Feb 15;91(4):236-42. PMID: 25955624.
On average, approximately 1300 Americans die of hypothermia each year
These don’t all occur in cold mountain regions. Homelessness, mental illness and substance abuse are important risk factors, particularly in urban areas.
Not all hypothermia cases are related to exposure! Other causes include hypoglycemia, hypothyroidism, hypoadrenalism, hypopituitarism, CNS dysfunction, drug intoxication, sepsis and dermal disease
Hypothermia = core body temperature < 35 degrees C (95 degrees F)
Mild hypothermia (32-35 degrees C): present with shivering, tachycardia, tachypnea and hypertension
< 32 degrees C: shivering stops and HR and BP decrease; patients become confused, lethargic and then comatose; Reflexes are lost, RR increases; bronchorrea occurs; aspiration is common; cold diuresis and hemoconcentration occur
As temp lowers, sinus bradycardia develops into atrial fibrillation with slow ventricular response to ventricular fibrillation to asystole. At temps < 30 degrees C, the risk for dysrhythmias increases
Rewarming and Management
Type of rewarming is based on cardiovascular status, NOT temperature
Passive rewarming: removal from cold environment and wet clothes, insulation
Active external rewarming: warm water immersion, heating blankets set at 40 degrees C, radiant heat, forced air
Active core rewarming at 40 degrees C: Inhalation rewarming (warm air via the vent), heated IV fluids, GI tract lavage, bladder lavage, peritoneal lavage, pleural lavage, extracorporeal rewarming, mediastinal lavage by thoracotomy
Remember to handle these patients gently to avoid precipitation of ventricular fibrillation!
ECMO in Hypothermic Arrest
The use of ECMO has been recommended as the rescue therapy of choice for hypothermic cardiac arrest for its ability to rapidly rewarm patients (8-12 degrees/hour) and provide complete cardiopulmonary support
Studies have shown that patients with cardiac arrest have a rate of survival of 50% with the use of ECMO, whereas, at centers without ECMO, these same types of patients have a survival rate of only 10%
Cases of survival with a good clinical outcome have been reported with core temperatures as low as 13 degrees Celsius and in cases requiring long transport with more than 5 hours of CPR!
Risk Factors for Poor Prognosis Despite Aggressive Therapy (ECMO, etc):
Clear history of cardiac arrest before cooling
Obvious signs of irreversible death
Core body temperature higher than 32 degrees Celsius with asystole
Flint LA, David DJ, Smith AK. Rehabbed to Death. N Engl J Med. 2019;380(5):408-409. doi:10.1056/NEJMp1809354
Flint LA, David D, Lynn J, Smith AK. Rehabbed to Death: Breaking the Cycle. J Am Geriatr Soc. 2019;67(11):2398-2401. doi:10.1111/jgs.16128
Burke RE, Jones J, Lawrence E, et al. Evaluating the Quality of Patient Decision-Making Regarding Post-Acute Care. J Gen Intern Med. 2018;33(5):678-684. doi:10.1007/s11606-017-4298-1
Halifax E, Bui NM, Hunt LJ, Stephens CE. Transitioning to Life in a Nursing Home: The Potential Role of Palliative Care. J Palliat Care. 2021 Jan;36(1):61-65. doi: 10.1177/0825859720904802. Epub 2020 Feb 27. PMID: 32106767; PMCID: PMC8127871.
Makdisi G, Wang IW. Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. J Thorac Dis. 2015;7(7):E166-E176. doi:10.3978/j.issn.2072-1439.2015.07.17