")


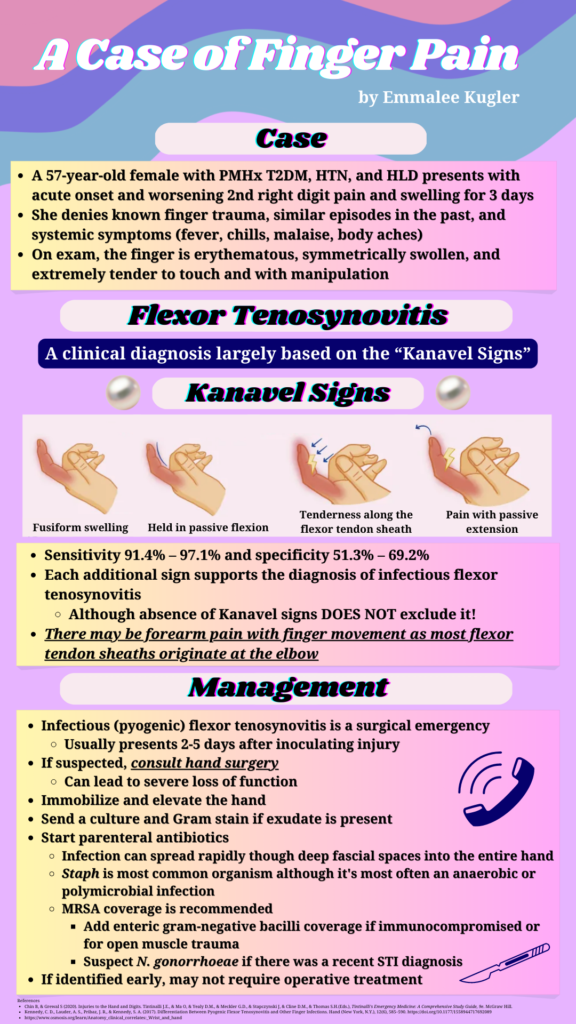
An unidentified male estimated to be approximately 20 years old presents via EMS shortly after a gunshot wound to the leg. Upon arrival, he is belligerent, uncooperative with care, and subsequently intubated. Exam shows a penetrating wound to the left anterior thigh with copious pulsatile bleeding. His extremities are cool with diminished pulses throughout. FAST is negative. A compression bandage is applied. Vital signs after 1 unit of packed red blood cells are: HR 150, BP 74/52, RR 16, SpO2 99% on 40% FiO2. At this time, which of the following is indicated for the management of this patient?
A: CT angiogram of the extremity
B: intravenous tranexamic acid
C: norepinephrine infusion
D: platelet transfusion
Answer: intravenous tranexamic acid
This patient is in hemorrhagic shock secondary to an arterial injury from a gunshot wound. The CRASH-2 trial in 2010 demonstrated that administration of intravenous tranexamic acid within 3 hours of injury for adult trauma patients with significant bleeding decreases mortality when compared to placebo. The patient is unstable with hard signs of vascular injury and should be taken immediately to the operating room. Definitive management should not be delayed for imaging. Norepinephrine and other vasopressors are not indicated as the patient is already vasoconstricted from volume loss. Additional units of packed red blood cells, not platelets, are more appropriate at this time as he is being prepared for surgical exploration and repair.
| Hard Signs of Vascular Injury (ABCDE) |
| Active pulsatile hemorrhage |
| Bruit or palpable thrill |
| Can’t feel distal pulse |
| Distal ischemia |
| Expanding hematoma |
References:
CRASH-2 trial collaborators, Shakur, H., Roberts, I., Bautista, R., Caballero, J., Coats, T., Dewan, Y., El-Sayed, H., Gogichaishvili, T., Gupta, S., Herrera, J., Hunt, B., Iribhogbe, P., Izurieta, M., Khamis, H., Komolafe, E., Marrero, M. A., Mejía-Mantilla, J., Miranda, J., Morales, C., … Yutthakasemsunt, S. (2010). Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet (London, England), 376(9734), 23–32. https://doi.org/10.1016/S0140-6736(10)60835-5