

")



Vasopressors Part V: Dopamine

Case: An 80 year old female with a history of COPD presents to the hospital after a fall from standing onto her right side with respiratory distress. She repeatedly states feeling pressure to her face and “my face feels tight”. She appears to be in respiratory distress and is intubated for airway protection. Exam is notable for mild decreased breath sounds BL and for crepitus across her chest, bilateral arms, face, and back. You get a chest X-ray followed which is shown below.
What is the diagnosis? What is the name of the radiologic finding on CXR?


Diagnosis:

Resources:
Fahrenhorst-Jones, Travis. “Ginkgo Leaf Sign (Subcutaneous Emphysema): Radiology Reference Article.” Radiopaedia, Radiopaedia.org, 17 May 2022, radiopaedia.org/articles/ginkgo-leaf-sign-subcutaneous-emphysema?lang=us.
Kukuruza, Kelsey, and Ayham Aboeed. “Subcutaneous Emphysema .” StatPearls, www.ncbi.nlm.nih.gov/books/NBK542192/.
Sean Coulson D.O.
HPI: Pt is a 24 y/o male who presents for fall, complaining of right lateral anterior palm pain. No medical hx, TDap up to date, no anticoagulation.
Physical Exam: Tender to palpation over the medial right palm on the anterior aspect. Radial pulse 2+, Cap refill intact, Strength and sensation intact, no abrasions / lacerations / skin changes. When the patient closes the right hand and makes a fist, the right 2nd finger angulates and bends overtop the 3rd phalanx (as seen below).
Pertinent Information About 2nd-5th Metacarpal Fractures:
Is it an open vs closed? Does it involve the intra articular space? Cascade of finger placement, malrotation / scissoring (see photo below)?
What are acceptable degrees of angulation based on the digit?
1st metacarpal: < 10 degrees
2nd: <20 degrees
3rd: < 30 degrees
4th: < 40 degrees
If less than the stated degree, may consider reduction, splint and discharge with orthopedic follow up if no other concerning features are present.


Other Indications for operative management and in ED orthopedic consult
Angulation greater than what’s stated above
Shortening > 5mm
Intraarticular or open fracture
Abnormal finger cascade regardless of degree of angulation
Multiple metacarpal fx
Management
+/- Ortho evaluations w/ operative fixation as described above
4th / 5th MCP fx: ulnar gutter splint
2nd / 3rd MCP fx: radial gutter splint
References:
https://www.ncbi.nlm.nih.gov/books/NBK551532
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7355092
https://www.journal-cot.com/article/S0976-5662(20)30230-7/fulltext

References:
https://www.ncbi.nlm.nih.gov/books/NBK482160
https://cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines/algorithms
https://www.ncbi.nlm.nih.gov/books/NBK482124
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8139870
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5367766
https://www.emrap.org/corependium/drug/recLg1S2Jxb7XHuBZ/Epinephrine#h.isp1462n5h9n

A 20 y.o patient presents to the ED after a motor vehicle accident after hitting a ditch. He is fully alert and oriented and is reporting generalized abdominal pain and myalgias. Physical exam is notable for diffuse abdominal tenderness, seatbelt sign with bruising to the right upper chest wall and right flank. VS: HR 70, BP 108/59, RR 18, SpO2 99%
A FAST exam is performed which demonstrates the following:
A CT scan was subsequently performed which confirmed large volume hemoperitoneum with a grade 2 liver laceration.

The patient was subsequently taken to the OR for an exploratory laparotomy. He was ultimately stabilized, and was able to be discharged from the hospital 2 weeks later.
Focused Assessment with Sonography in Trauma: FAST
Resources:
Netherton, Stuart, et al. “Diagnostic accuracy of Efast in the trauma patient: A systematic review and meta-analysis.” CJEM, vol. 21, no. 6, 18 July 2019, pp. 727–738, https://doi.org/10.1017/cem.2019.381.
Alyssa Exarchakis, MS4






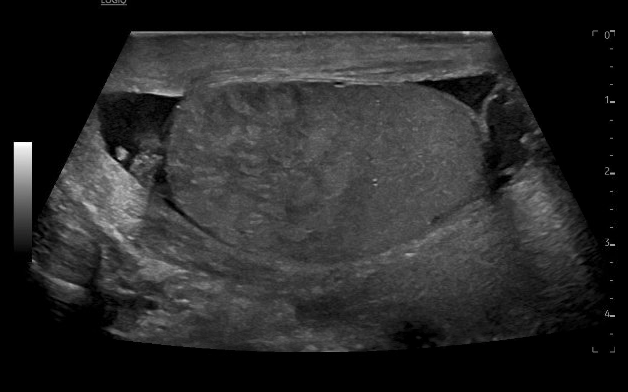
65 year old M presents with significant swelling, discoloration and pain to the right scrotum and penis after inguinal hernia repair 2 days prior. On exam, patient with ecchymosis and erythema of the right testicle and shaft of the penis. There is significant swelling in the inguinal canal, which is not compressible or reducible. You take the ultrasound to bedside to see:
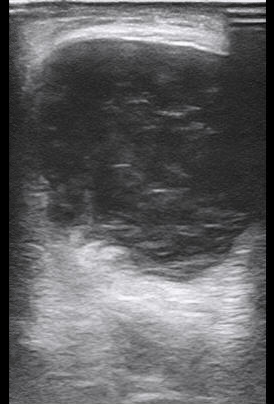

What is the diagnosis?
Answer: Scrotal hematoma
Differentials for this patient include hematoma, hydrocele, scrotal abscess or infection, failure of mesh causing strangulated or incarcerated hernia.
On imaging, you see mixed echogenic fluid collection with no vascular flow noted. This extends from the right groin into the scrotum, with hypoechogenic fluid tracking around bilateral testicles. This is consistent with a scrotal hematoma. There is no bowel noted, ruling out strangulated or incarcerated hernia. There is no “swirl” sign which would be more consistent with scrotal abscess/infection. The mixed echogenic fluid is most consistent with hematoma rather than hydrocele.
Pearls for the bedside scrotal ultrasound:
References:
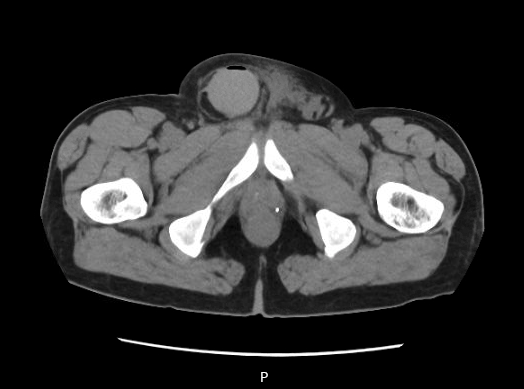
CT and radiology ultrasound imaging from case are below:
Pt is a 55 y/o F w/ hx of SLE who presents to the ED for hypotension. Pt is altered and not providing any information. Pt arrives with family who notes she has had progressively worsening mental status and abdominal pain w/ vomiting non bilious material x 3 days. Not compliant with medications during this time 2/2 vomiting. Unclear what medications she takes.
HR 119, BP 71/48, Temp 94F, RR 20, Acc Check 51
Physical Exam:
GCS 11, arousable to gentle stimuli
Extremities warm w/o pitting edema
Abdomen soft and nontender
Lungs CTA b/l
Heart rate tachycardia and regular
POCUS unremarkable
Pertinent Labs:
CBC: WBC 15k w/ increased lymphocytosis
BMP: Na 128, K 5.8, AG 18, Cr 2.1
Differential diagnosis: Distributive shock 2/2 sepsis w/ unclear source vs adrenal insufficiency, hypovolemia, myxedema coma etc.
Physiology
When to consider
High Risk Groups
Diagnosis
Management
Prevention
References: