Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. Tintinalli J.E., & Ma O, & Yealy D.M., & Meckler G.D., & Stapczynski J, & Cline D.M., & Thomas S.H.(Eds.),Eds.
EMRap compendium
Konca C, Kahramaner Z, Bosnak M, Kocamaz H. Hemlock (Conium Maculatum) Poisoning In A Child. Turk J Emerg Med. 2016 Feb 26;14(1):34-6. doi: 10.5505/1304.7361.2013.23500. PMID: 27331163; PMCID: PMC4909876.
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. Tintinalli J.E., & Ma O, & Yealy D.M., & Meckler G.D., & Stapczynski J, & Cline D.M., & Thomas S.H.(Eds.),Eds.
EMRap compendium
Horowitz KM, Kong EL, Regina AC, et al. Gyromitra Mushroom Toxicity. [Updated 2024 Feb 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470580/
Tobias M, McGoldrick M, Rometti M, Laub J, Wei G, Fernandez D. Diagnosis and Management of Amanita Phalloides Toxicity in the Emergency Department Observation Unit: A Case Report. Clin Pract Cases Emerg Med. 2024 Feb;8(1):49-52. doi: 10.5811/cpcem.1268. PMID: 38546312; PMCID: PMC10966493.
12-month-old who was born full term is brought in by mom after patient was found to be cyanotic. Patient with vaccines UTD. Patient has been teething and mom notes that she has been applying benzocaine teething gel. Patient on arrival to the ER has perioral and digital cyanosis. His vital signs are as follows: T- 98.6 rectal; HR- 140; RR- 35; BP- 94/56; SpO2- 89% on RA. Patient is given blow by O2 with no improvement to oxygenation. What is the diagnosis?
Patent Foramen Ovale
Aspirin Toxicity
Methemoglobinemia
Iron toxicity
Carbon monoxide poisoning
Answer: C. Methemoglobinemia
Patient has methemoglobinemia from the application of benzocaine for teething. Methemoglobinemia occurs when iron is oxidized from the ferrous (Fe2+) to the ferric (Fe3+) state. The ferric hemes of the methemoglobin do not bind O2. The ferric heme in the hemoglobin also has an increased affinity to O2 and therefore causes the hemoglobin dissociation curve to shift to the left causing less oxygen delivery.
A 65 year old male with a past medical history of type 2 diabetes and hyperlipidemia presents via EMS as a stroke alert. Patient developed confused speech and right upper extremity weakness 1 hour ago. Vital signs and point of care glucose are within normal limits. CT head and CTA head and neck demonstrate no acute intracranial abnormalities, and thrombolytics are administered. Ten minutes later, the patient develops rapidly progressive tongue and lip swelling. There is no response to intramuscular epinephrine. What is the likely etiology of the patient’s change in condition?
A: Hemorrhagic transformation
B: IgE-mediated hypersensitivity to thrombolytics
C: Mast cell activation from IV contrast
D: Thrombolytic side effect
Answer: D. Thrombolytic side effect
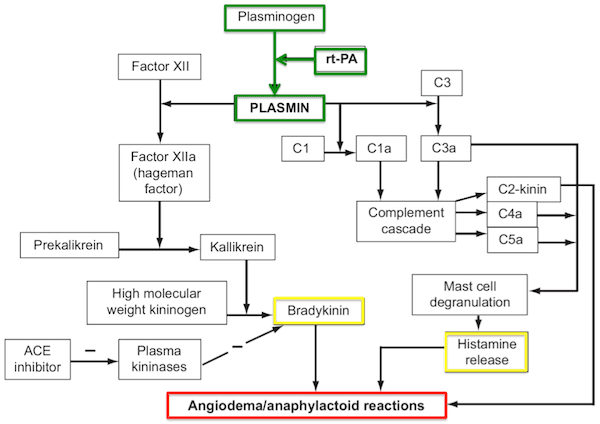
This patient is most likely experiencing orolingual angioedema, a known side effect of thrombolysis that is overall rare but in some reports has an incidence as high as 17%. It is caused by complement and kinin pathway activation by plasminogen. Patients who are already taking ACE inhibitors are at increased risk. Treatment involves discontinuing thrombolysis and managing similarly to other causes of angioedema.
It is unlikely that intracranial hemorrhage would cause airway swelling. IgE-mediated hypersensitivity reactions require an initial sensitization exposure which makes this answer unlikely without prior administration of thrombolytics. Mast cell activation from IV contrast is possible but would likely have response to intramuscular epinephrine in addition to other physical exam findings such as urticaria or wheezing.
References:
Go S, Kornegay J. Stroke Syndromes. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.



")