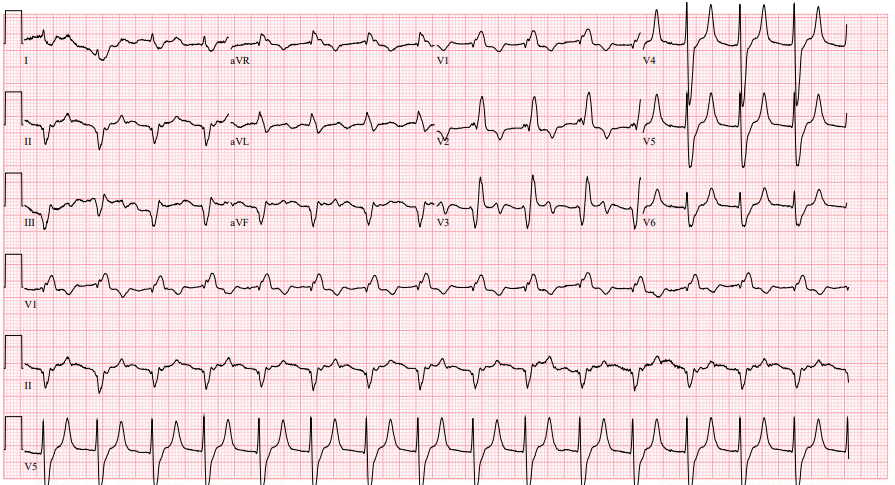
A 70 year old male with a past medical history of hypertension, type 2 diabetes, and atrial fibrillation on warfarin presents for visual changes. He is accompanied by his daughter who states that about one hour ago, his vision on the right side became blurry. There is associated right facial numbness and headache. His daughter believes that he has become more confused over this time period. Fingerstick glucose is 220. An EKG is obtained which shows atrial fibrillation at a rate of 92.
Exam
BP 151/75, HR 92, T 97.8F, RR 18, SpO2 98%
Comfortable appearing in no acute distress. GCS E4 V4 M6. No facial droop. Decreased sensation to right side of face. 5/5 strength and sensation in all extremities. No difficulty with rapid alternating movements. Extraocular motion intact. Left gaze preference with right sided homonymous hemianopia.
Case continued: Neurology is emergently consulted and a stroke alert is activated. CT/CTA of the head and neck shows no acute intracranial hemorrhage and no large vessel occlusion. Labs are notable for an INR of 1.6. The decision is made in conjunction with neurology to administer thrombolytics, and the patient is admitted to neurology critical care. Repeat head CT 24 hours later demonstrates a left parieto-occiptal infarct.
Pearls:
– This patient’s neurologic deficits including right sided facial numbness, right homonymous hemianopsia, left sided gaze preference, and aphasia localize to a cortical distribution as noted above.
– Warfarin use alone is not a contraindication to thrombolytics for acute ischemic stroke. The INR must be > 1.7 in addition to be an exclusion criterion.
– This patient had multiple previous subtherapeutic outpatient INR levels which likely precipitated an embolic stroke.
– In patients without contraindications, the decision to administer thrombolytics for acute ischemic stroke should be clinical without waiting for results of laboratory testing with the exception of a point of care glucose and patients with suspected coagulopathy.
– Other common exclusion criteria to use of thrombolytics in acute ischemic stroke include previous head trauma or stroke within 3 months, any previous intracranial hemorrhage, SBP > 185 or DBP > 110, or known intracranial mass such as neoplasm or aneurysm.
References:
Go S, Kornegay J. Stroke Syndromes. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e.
Powers WJ, Rabinstein AA, Ackerson T, et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association [published correction appears in Stroke. 2018 Mar;49(3):e138] [published correction appears in Stroke. 2018 Apr 18;:]. Stroke.
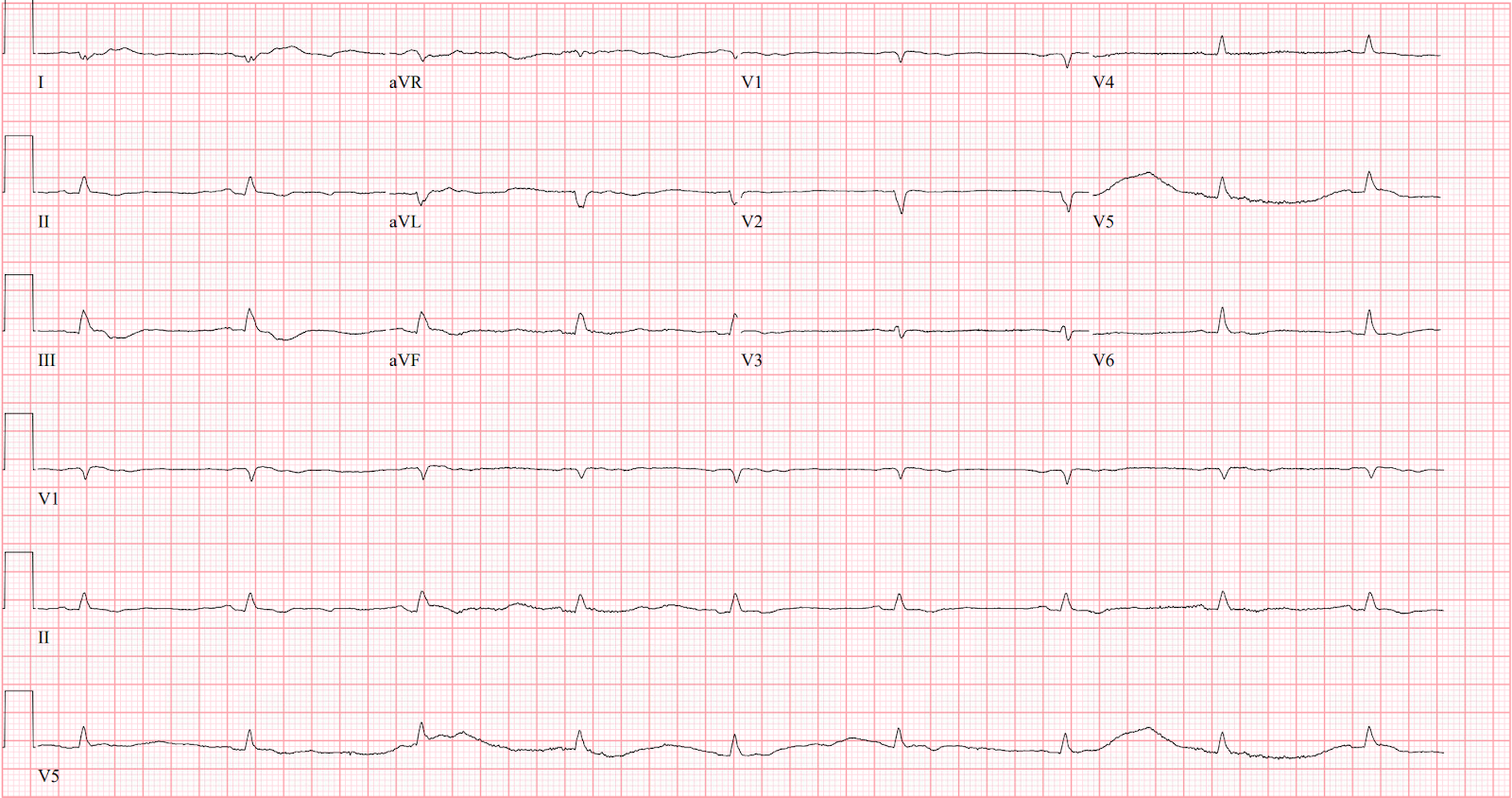
HPI: A 29 year old male with a past medical history of polysubstance use presents to the ED in December via EMS for a suspected overdose. History is limited due to patient cooperation. EMS states that he was found outside in a puddle, minimally responsive. He was given 2mg IM naloxone by EMS and became acutely agitated and combative afterward, requiring 5mg IM midazolam and 5mg IM haloperidol upon arrival. Fingerstick glucose 226. ECG is obtained and shown below.
Exam: BP 182/84, HR 111, T 86.1F, RR 18, SpO2 100%
Disheveled appearing male in wet clothes, intermittently thrashing. Cold to touch. Pupils 5mm bilaterally. No signs of trauma. GCS E3 V2 M5. Moves all extremities equally. Heart rate is tachycardic and irregular
ECG interpretation: atrial fibrillation with Osborne waves
Differential diagnosis: polysubstance use, environmental cold exposure, severe sepsis, hypothyroidism
Case continued: Active rewarming is initiated by removing wet clothes, administering warmed IV fluids, and placing a bair hugger. Labs are notable for a creatinine kinase of 3966. The patient’s temperature, heart rate, and mental status significantly improve within 5 hours, and his repeat EKG shows normal sinus rhythm without Osborn waves. He is ultimately admitted to medicine.
Pearls:
– The cardiovascular response to cold is peripheral vasoconstriction and initial increase in heart rate and blood pressure. As core temperature drops below 32C, there is myocardial irritability and risk of cardiovascular collapse.
o Atrial fibrillation and flutter are common arrhythmias associated with hypothermia.
o Rescue collapse is a term to describe cardiac arrest that occurs during extrication or transport of a profoundly hypothermic patient due to profound myocardial irritability.
– Osborn waves are positive deflections at the end of the QRS complex that are non-specific but may occur in temperatures below 32C.
o Size of the wave correlates with the degree of hypothermia but has no prognostic value.
– As temperature continues to drop, EKG changes are variable but classically include bradycardia with prolonged PR, QRS, and QTc. Heart block or ventricular dysrhythmias may be encountered as well. Asystole is the common final dysrhythmia.
– Rewarming is the treatment of choice.
o Atrial dysrhythmias such as atrial fibrillation will often resolve with warming.
o Cardioversion for unstable arrhythmias should be attempted but may be refractory in severe hypothermia.
References:
Brown DA. Hypothermia. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
Hoek T. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010. 122:5829-5861
22 yo male hx of prior GSW to L chest with retained bullet presents with chief complaint of 2 days of left sided chest and left upper quadrant abdominal pain, along with intermittent nonbilious emesis
No fevers, no dyspnea, normal bowel movements
Physical Exam
VS: T 97.3 HR 80 BP 153/70 O2 98% on RA
Well appearing, in no distress
Lungs clear bilaterally, heart sounds normal
Abdomen soft, +tenderness in LUQ without guarding and rebound tenderness
No lower extremity edema
ECG:
Chest film:
Interpretation: Apparent left sided pleural effusion, not apparent on lateral view
CT chest:
Highlighted area indicates diaphragmatic hernia with portion of the stomach in the left chest
Clinical Course
NGT placed to decompress stomach
Admitted to CT surgery
Had EGD to assess viability of gastric mucosa which was normal
Underwent open surgical repair of diphragmatic hernia with reduction of stomach into abdominal cavity
Pearls
Diaphragmatic hernia is a rare condition usually a sequelae of trauma
Conventional imaging such as CT will likely not detect an acute injury to the diphragm
Patients often present late after acute trauma when visceral contents herniate into the chest cavity
Exam may demonstrate acute respiratory distress and bowel sounds on pulmonary auscultation
Patients may be in frank shock from gastric/intestinal ischemia
A 60 year old male with a PMH of DM, HTN, HLD, MI presents to the ED after being found down with waxing and waning mentation. The patient complains of abdominal pain and diffuse myalgias.
BP 76/56, HR 92, Temp 98.4F, RR 22.
Physical exam
Pressure wounds of the right rib cage, right side of his forehead
Right calf tenderness with a firm anterior compartment, cool/pale right lower extremity, dorsalis pedis and posterior tibial pulses were unable to be palpated.
ECG:
ECG interpretation: Peaked T waves, widened QRS concerning for hyperkalemia
Clinical course:
1L bolus of LR
IV calcium gluconate for possible hyperkalemia
Surgery was immediately consulted due to concern for compartment syndrome
Labs were notable for a potassium of 7.2, creatinine of 3.49, creatinine kinase of 188,760, a lactate of 4.0, and ALT/AST in the 3,000s/5,000s
Given intermittent hemodynamic instability a dialysis line was placed for definitive hyperkalemia management
Patient underwent emergent lower extremity fasciotomy with surgery
Compartment syndrome learning points:
· Diagnosis is both clinical and by compartment pressure measurements
· Compartment pressure >30mmHg or a delta pressure <30mmHg (diastolic BP – compartment pressure) is diagnostic
· Clinical findings: 6Ps. Pain is the earliest and often only symptom, the rest are late findings.
o Pain out of proportion to the exam (most common finding)
o Pallor
o Paresthesia
o Paresis/paralysis
o Pulselessness
o Poikilothermia
· Management: Immediate surgical consult for fasciotomy
Today’s case from the EM Daily archives involves one of the rare patients where you DO want to acutely treat elevated blood pressure with intravenous agents….
HPI
48 year old male with PMH HTN presents with blurry vision for 2.5 hours
Patient was using the computer tonight, could not see where the icons were on his desktop, could still see light/colors.
He has no pain in his eyes
Also reports dyspnea on exertion for 2 days. No headache, no chest pain, no abdominal pain
He has not had his anti-hypertensives (he reports he is on 5 different medications) for about 1.5 weeks
Physical Exam
T 98.3 BP 290/120, HR 118, RR 18, SpO2 99%
Patient is awake, alert, conversant, appears well and in no distress
Neuro: Visual acuity 20/200 OS, OD, OU Normal visual fields Normal pupillary exam Normal extraocular movements Otherwise normal cranial nerve exam Normal strenght in extremities , no pronator drift, normal finger to nose
Cardiac: tachycardic, normal S1/S1, no murmurs/rubs/gallops
Pulm: clear to auscultation bilaterally
Abdomen: soft, nontender, nondistended
Differential Diagnosis
Hypertensive emergency with elevated BP and evidence of end organ damage (decreased visual acuity, evidence of pulmonary edema on bedside US)
Sympathomimetic toxicity (hypertension, tachycardia), though patient reports no ingestions of medications or drugs
Thyrotoxicosis
CVA given visual changes, however with no focal visual deficits (no visual field cut, decreased acuity is symmetric bilaterally)
Initial ED Management
Arterial line place – IV nicardipine started, with goal SBP 210s (25% reduction in the first hour)
Bedside lung US performed which demonstrates numerous B lines consistent with evolving pulmonary edema
Labs/Imaging –
Hb 6.1, PLT 142, WBC 5.92 – Na 147, K 3.7 – Cr 15.03 (last level in chart 3.95 7 years ago) – HS troponin 223 – pro-BNP 26,930
CT Head with 3 small, distinct areas of intraparenchymal hemorrhage
Further Management
Repeat neurologic exam performed and is unchanged
Neurosurgery consulted, recommend BP goal under SBP 160
Repeat CTH in 4 hours: unchanged
Patient admitted to ICU for IV nicardipine, continuous BP monitoring, and q1 hour neuro checks
Pearls
Hypertensive emergency is acute SBP over 180 with evidence of organ dysfunction
Not every patient with SBP over 180 requires emergency BP control
In this patient: decreased visual acuity, pulmonary edema, elevated troponin and proBNP, renal failure, and intraparenchymal hemorrhage = hypertensive emergency
In managing hypertensive emergency, SBP should not be lowered by more than 25% in the first hour to prevent causing hypoperfusion and cerebral ischemia
Continuous BP monitoring via arterial line is important to carefully titrate medications
Nicardepene is an easy to titrate CCB which may be the ideal agent for the treatment of hypertensive emergency
Indications for emergent dialysis (AEIOU – acidosis, electrolytes, intoxication, overload, uremia): critical metabolic acidosis, refractory or rapidly increasing hyperkalemia, life threatening intoxication with substance that is able to be removed with HD, volume overload, complications of uremia (pericarditis, neuropathy, encephalopathy)
53 y/o male p/w complaints of L eyelid swelling and redness
Started 4 days PTA as small pimple which he popped, and slowly progressed to “softball” sized area of swelling with pus drainage
Subjective fevers
Physical Exam
BP 153/90, pulse 80, temp 98.6, RR 17
PERRL, EOMI
Extensive soft tissue erythema and edema of the L upper eyelid, 5×5 area of fluctuance with active pus draining from small laceration
Visual acuity: 20/40 R, 20/70 L
No corneal abrasions or ulceration on fluorescein staining
IOP 21 bilaterally
DDx
Preseptal / periorbital cellulitis
Orbital cellulitis
Abscess
Workup
Labs: CBC, BMP, lactate, wound culture
Started empirically on broad spectrum abx: 2g vancomycin + 3g unasyn
CT orbits w/ contrast: significant soft tissue swelling of the L periorbital region consistent with inflammatory/infectious process, and involvement of the medial orbital wall along the lamina papyracea
Clinical Course
Admission for continued IV antibiotics
Repeat CT orbits
Consults: OMFS, ophthalmology, ENT, ID
Take home points
MUST differentiate orbital vs preseptal cellulitis given the increased morbidity and mortality a/w orbital (see table)
Confirm clinical suspicion with CT imaging
Orbital cellulitis complications: subperiosteal abscess, orbital abscess, vision loss, cavernous sinus thrombophlebitis, and/or brain abscess
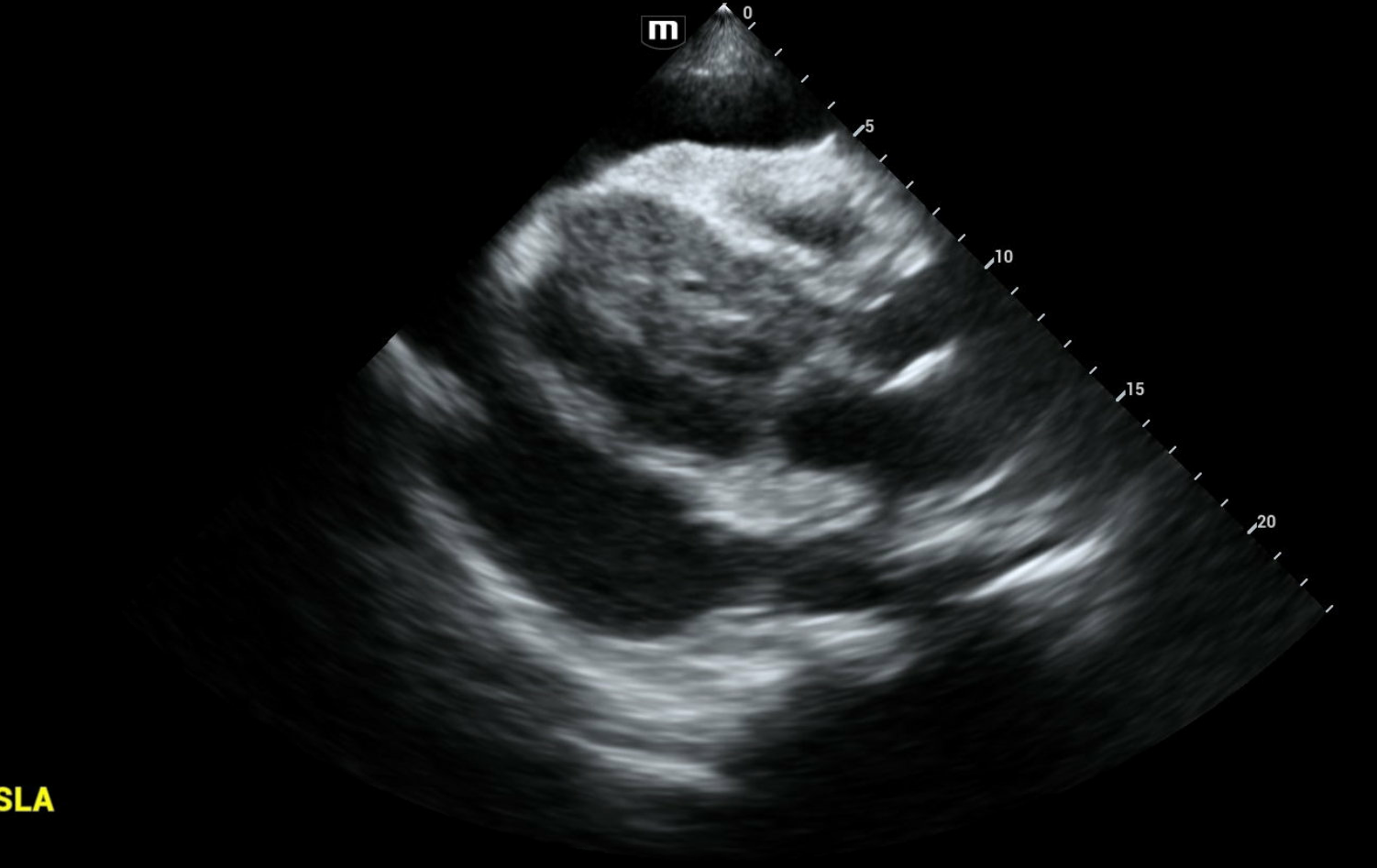
52 year old female with pmhx of hypothyroidism who presents to Emergency Department with bilateral leg swelling and SOB with exertion. Reports swelling began one week ago and has progressively worsened. Denies any other symptoms. Patient has not seen a cardiologist/had an echo performed before. Reports she has not taken her prescribed levothyroxine for two years now.
For a FANTASTIC review of ultrasound guided emergency pericardiocentesis, check out the Ultrasound Podcast Youtube video HERE
Case continued:
Patient found to be hypoglycemic at 50 mg/dL, D10 administered
Patient found to be hyponatremic at 125, likely in setting of fluid overload
Cardiology consulted for cardiac tamponade, pericardiocentesis performed with 1.4 L drained.
Ascites drained via paracentesis, other diagnoses ruled out with hypothyroidism most likely cause.
Patient restarted on levothyroxine and began liothyronine (T3)in hospital
Patient discharged home in stable condition after 10 days in hospital with levothyroxine, has not returned to hospital since
Pearls:
Consider hypothyroidism if patient has pmhx or classical physical exam findings: bradycardia, hypothermia, hypotension, lethargy, constipation, hair loss/thinning, facial swelling, coarse skin, pretibial myxedema(thickened, nonpitting edema), menstrual changes, decreased reflexes.
Hypothyroidism increases permeability in the blood vessels of the body and decreases drainage of lymphatic system, causing an accumulation of fluid outside of blood vessels and can present as pretibial myxedema, pericardial effusion, or pleural effusion.
Precipitating factors of hypothyroidism include medication nonadherence, infection, cold exposure, stroke, autoimmune disorders, thyroid radiation/surgery, and medications (amiodarone, lithium).
Management of hypothyroidism includes supportive, hydrocortisone(prevents adrenal crisis), levothyroxine (T4) and +/- Liothyronine (T3) supplementation.
References:
Chahine J, Ala CK, Gentry JL, et al Pericardial diseases in patients with hypothyroidism Heart 2019;105:1027-1033.
Patil N, Rehman A, Jialal I. Hypothyroidism. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519536/
69 year-old female with a past medical history of ESRD on HD, HIV, Pulmonary HTN, HFrEF (EF 25%), anemia, thrombocytopenia presents after dialysis with left upper extremity pain and swelling. The dialysis RN reports there was shiny skin present over the LUE AVF and they cannulated to avoid that area, the patient received one hour of treatment that was stopped due to pain. Patient reports the her arm above the AVF has been slowly enlarging
Vitals
BP: 98/54, HR: 78, RR 20, T: 97.6
Exam:
Alert and oriented, no acute distress, chronically-ill appearing
LUE with no external bleeding, fistula has a palpable thrill. Swelling and tenderness are present above the AVF, over the medial upper arm.
Cap refill >2 seconds
Rest of exam unremarkable
Clinical Course
-CTA upper extremity was obtained to assess for active bleeding – showed AV fistula with aneurysmal dilatation, large hematoma with upper arm approximating a volume of 1000cc. No evidence of active hemorrhage
-Direct pressure was held above and below the AVF.
-Repeat BP 58/24
-Central line placed, resuscitated with 2U PRBC, 1 platelets, 1 FFP. Required norepinephrine and vasopressin drip
-Taken level 0 to OR for Brachiocephalic fistula ligation and hematoma evacuation with 500cc hematoma removed
-The patient was stabilized and recovered after being treated for hemorrhagic shock
Pearls
-AVF aneurysms can develop from repeated ruptures, increased venous pressure, and immunosuppression. They are usually asymptomatic, rarely rupture. Aneurysm formation is present in 5-7% of AVF
-Skin changes, pain, high output heart failure, and thrombosis can result from aneurysms and are an indication for operative management.
-AVF pseudoaneurysms can develop from extravasation of blood from cannulation sites, are more prone to rupture, develop more quickly
-Aneurysms/pseudoaneurysms can be identified by their shiny, thin, atrophic skin. In more severe cases can present with necrosis.
-Apply pressure and/or tourniquet above and below the AVF if life threatening hemorrhage is suspected
-Emergent consultation with vascular surgery warranted for operative repair
References:
Pasklinsky G, Meisner RJ, Labropoulos N, Leon L, Gasparis AP, Landau D, Tassiopoulos AK, Pappas PJ. Management of true aneurysms of hemodialysis access fistulas. J Vasc Surg. 2011 May;53(5):1291-7. doi: 10.1016/j.jvs.2010.11.100. Epub 2011 Jan 26. PMID: 21276676.
Lok CE, Huber TS, Lee T, Shenoy S, Yevzlin AS, Abreo K, Allon M, Asif A, Astor BC, Glickman MH, Graham J, Moist LM, Rajan DK, Roberts C, Vachharajani TJ, Valentini RP; National Kidney Foundation. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am J Kidney Dis. 2020 Apr;75(4 Suppl 2):S1-S164. doi: 10.1053/j.ajkd.2019.12.001. Epub 2020 Mar 12. Erratum in: Am J Kidney Dis. 2021 Apr;77(4):551. PMID: 32778223.
Saeed F, Kousar N, Sinnakirouchenan R, Ramalingam VS, Johnson PB, Holley JL. Blood Loss through AV Fistula: A Case Report and Literature Review. Int J Nephrol. 2011;2011:350870. doi: 10.4061/2011/350870. Epub 2011 May 30. PMID: 21716705; PMCID: PMC3118665.