by Carlos Cevallos M.D.
Case:
A 60 year old male with a PMH of DM, HTN, HLD, MI presents to the ED after being found down with waxing and waning mentation. The patient complains of abdominal pain and diffuse myalgias.
BP 76/56, HR 92, Temp 98.4F, RR 22.
Physical exam
Pressure wounds of the right rib cage, right side of his forehead
Right calf tenderness with a firm anterior compartment, cool/pale right lower extremity, dorsalis pedis and posterior tibial pulses were unable to be palpated.
ECG:
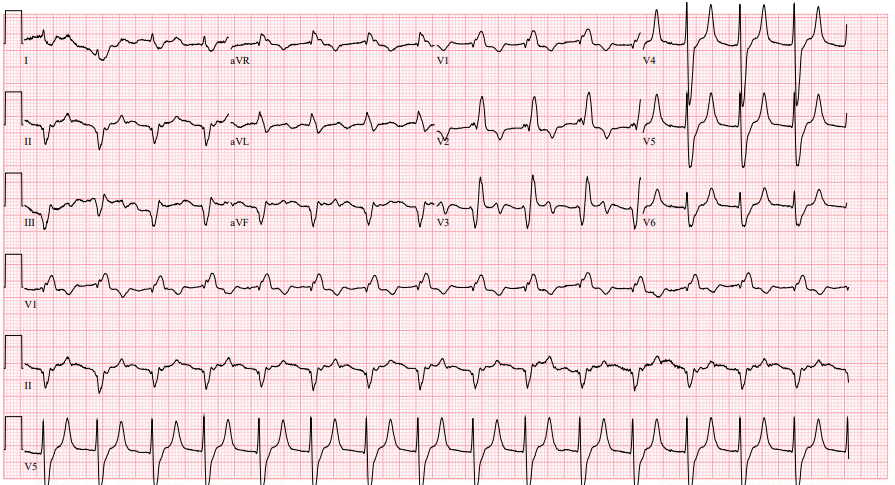
ECG interpretation: Peaked T waves, widened QRS concerning for hyperkalemia
Clinical course:
1L bolus of LR
IV calcium gluconate for possible hyperkalemia
Surgery was immediately consulted due to concern for compartment syndrome
Labs were notable for a potassium of 7.2, creatinine of 3.49, creatinine kinase of 188,760, a lactate of 4.0, and ALT/AST in the 3,000s/5,000s
Given intermittent hemodynamic instability a dialysis line was placed for definitive hyperkalemia management
Patient underwent emergent lower extremity fasciotomy with surgery
Compartment syndrome learning points:
· Diagnosis is both clinical and by compartment pressure measurements
· Compartment pressure >30mmHg or a delta pressure <30mmHg (diastolic BP – compartment pressure) is diagnostic
· Clinical findings: 6Ps. Pain is the earliest and often only symptom, the rest are late findings.
o Pain out of proportion to the exam (most common finding)
o Pallor
o Paresthesia
o Paresis/paralysis
o Pulselessness
o Poikilothermia
· Management: Immediate surgical consult for fasciotomy