Case: A 4 day old female born at 36w1d via C-section presents for tachycardia. Father at bedside states that he placed a heart monitor on the patient and it read over 200 bpm. Patient was seen at urgent care and transferred to ED via ambulance. Baby has otherwise acting normally, eating frequently, making 6+ wet diapers per day. No prior medical history. No family history of abnormal heart rhythms. Vitals include BP 85/53, HR 300, Temp 97.5F, RR 50, SpO2 100%. Exam shows a well appearing, interactive neonate with tachycardia on auscultation.
Differential diagnosis: Arrhythmia, dehydration, anemia, infection, hyperthyroidism
EKG is obtained and shown below:
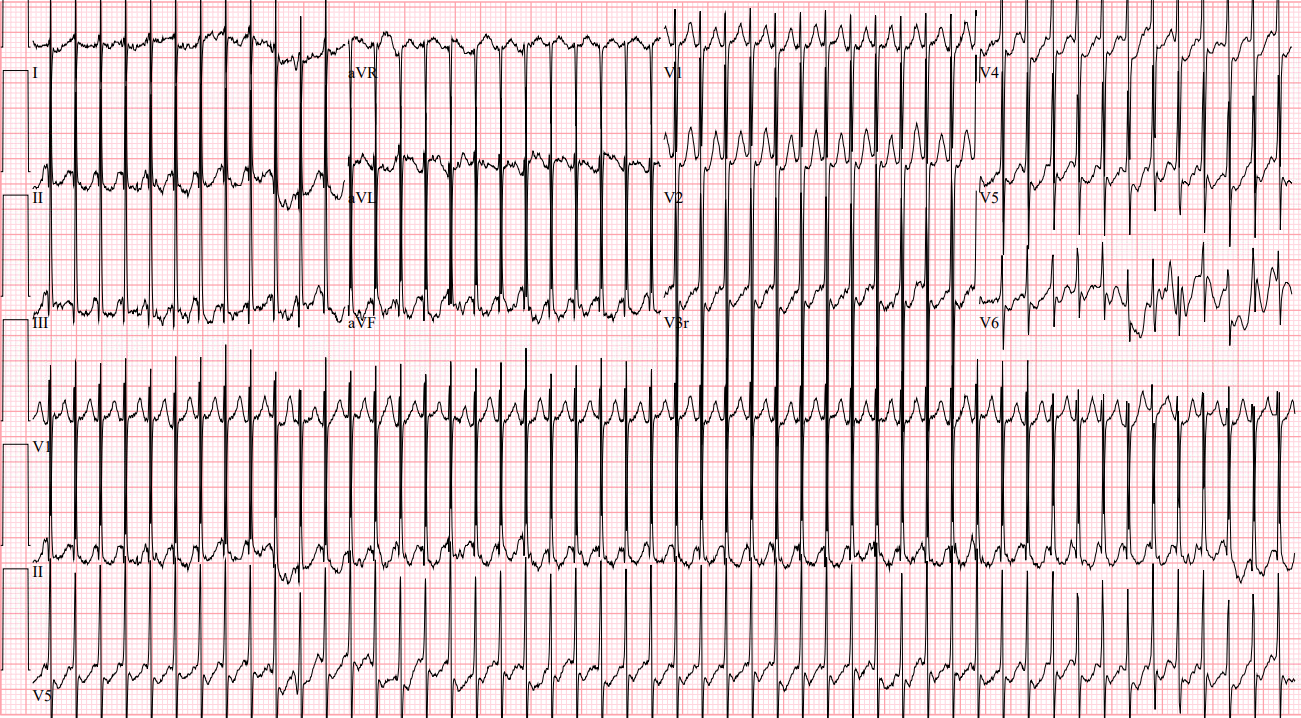
EKG interpretation: Supraventricular tachycardia at rate of 300
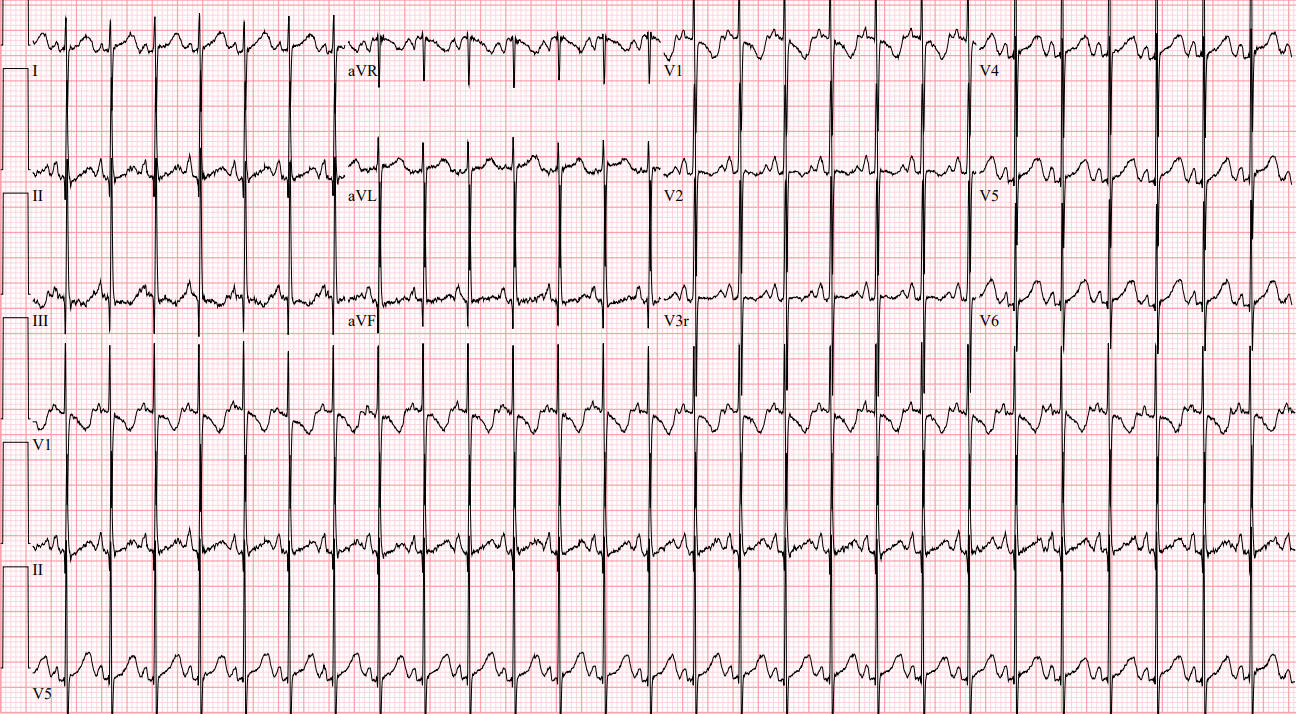
Case continued: Patient is placed on continuous cardiac monitoring. Vagal maneuvers are attempted including rectal temperature without success in terminating SVT. An IV is placed and adenosine is administered. Repeat EKG following adenosine is shown below. Pediatric cardiology is consulted and recommends administration of digoxin and transfer for further evaluation. Patient is then transferred to a pediatric center in stable condition.
Learning points:
- A heart rate > 220 bpm in an infant or > 180 bpm in a child with rate out of proportion to clinical status is likely supraventricular tachycardia.2
- Vagal maneuvers should be attempted initially for patients who are stable.
- Maneuvers that can be attempted in infants include obtaining a rectal temperature or applying a cold ice pack to the face to activate the mammalian diving reflex.
- If vagal maneuvers fail, rapid push of IV adenosine at a dose of 0.1 mg/kg is recommended.
- If the patient is unstable or adenosine fails to terminate the rhythm, perform synchronized cardioversion at a dose of 0.5-1 J/kg.
- Subsequent synchronized cardioversion attempts should be dosed at 2 J/kg.
References:
Hauda, II WE. Resuscitation of Children. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill Education; 2020.
Kleinman ME, Chameides L, Schexnayder SM, et al: Part 14: pediatric advanced life support. 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 122(18 suppl 3): S876, 2010. [PubMed: 20956230]