by Edward Guo M.D.
HPI
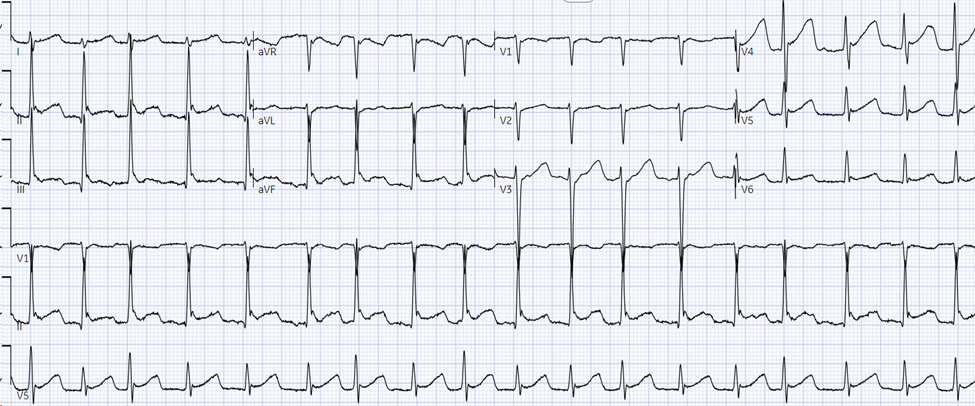
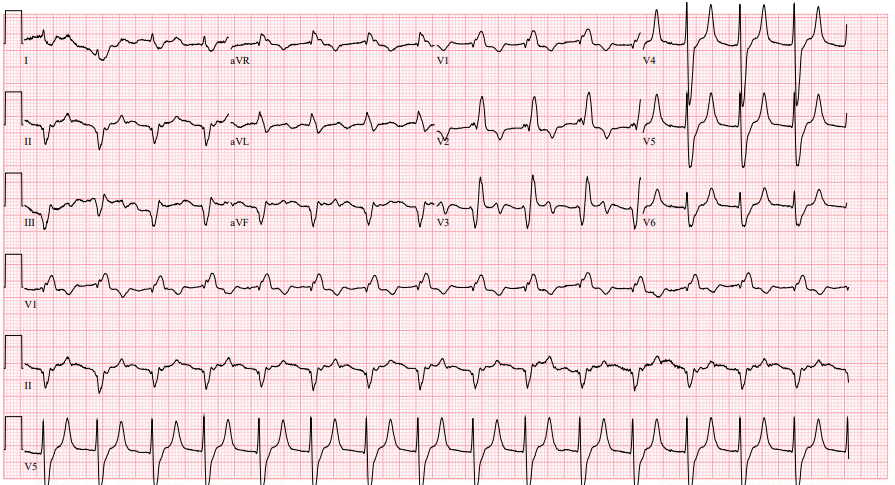
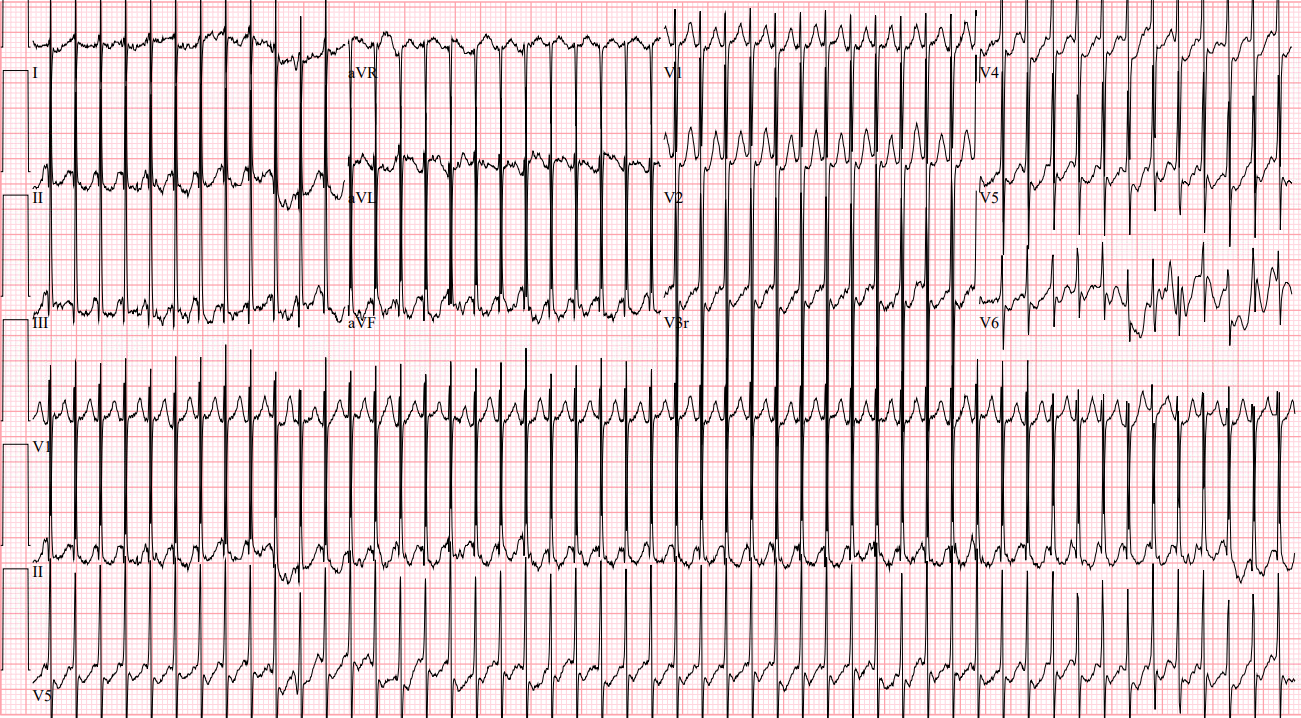
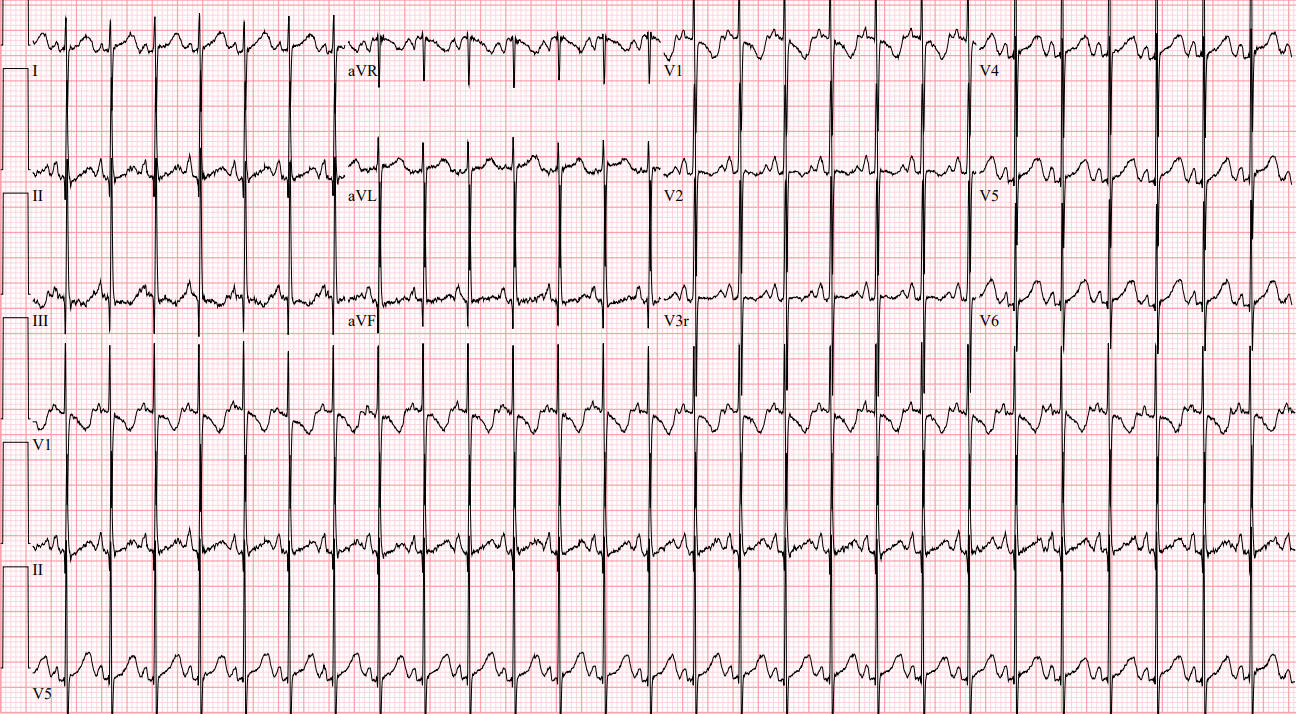
A 70 year old male with a past medical history of hypertension, type 2 diabetes, and atrial fibrillation on warfarin presents for visual changes. He is accompanied by his daughter who states that about one hour ago, his vision on the right side became blurry. There is associated right facial numbness and headache. His daughter believes that he has become more confused over this time period. Fingerstick glucose is 220. An EKG is obtained which shows atrial fibrillation at a rate of 92.
Exam
BP 151/75, HR 92, T 97.8F, RR 18, SpO2 98%
Comfortable appearing in no acute distress. GCS E4 V4 M6. No facial droop. Decreased sensation to right side of face. 5/5 strength and sensation in all extremities. No difficulty with rapid alternating movements. Extraocular motion intact. Left gaze preference with right sided homonymous hemianopia.
Differential diagnosis: acute ischemic stroke, spontaneous intracranial hemorrhage, complex migraine, toxic-metabolic encephalopathy
Case continued: Neurology is emergently consulted and a stroke alert is activated. CT/CTA of the head and neck shows no acute intracranial hemorrhage and no large vessel occlusion. Labs are notable for an INR of 1.6. The decision is made in conjunction with neurology to administer thrombolytics, and the patient is admitted to neurology critical care. Repeat head CT 24 hours later demonstrates a left parieto-occiptal infarct.
Pearls:
– This patient’s neurologic deficits including right sided facial numbness, right homonymous hemianopsia, left sided gaze preference, and aphasia localize to a cortical distribution as noted above.
– Warfarin use alone is not a contraindication to thrombolytics for acute ischemic stroke. The INR must be > 1.7 in addition to be an exclusion criterion.
– This patient had multiple previous subtherapeutic outpatient INR levels which likely precipitated an embolic stroke.
– In patients without contraindications, the decision to administer thrombolytics for acute ischemic stroke should be clinical without waiting for results of laboratory testing with the exception of a point of care glucose and patients with suspected coagulopathy.
– Other common exclusion criteria to use of thrombolytics in acute ischemic stroke include previous head trauma or stroke within 3 months, any previous intracranial hemorrhage, SBP > 185 or DBP > 110, or known intracranial mass such as neoplasm or aneurysm.
References:
Go S, Kornegay J. Stroke Syndromes. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e.
Powers WJ, Rabinstein AA, Ackerson T, et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association [published correction appears in Stroke. 2018 Mar;49(3):e138] [published correction appears in Stroke. 2018 Apr 18;:]. Stroke.