A 2 year old female with no past medical history presents for a nasal foreign body. The patient’s mother states that the child approached her earlier this evening while pointing at her nose. When the mother looked into the child’s right nostril, she noticed something metal. Vital signs are normal for age. On exam, the patient is in no acute distress with mucus coming from the right nostril and a silver metallic object lodged in the nare. A skull x-ray is obtained and shown below. The area of interest is included and zoomed in. What’s the diagnosis and what’s the appropriate management?

Answer: Nasal button battery – emergent removal in ED
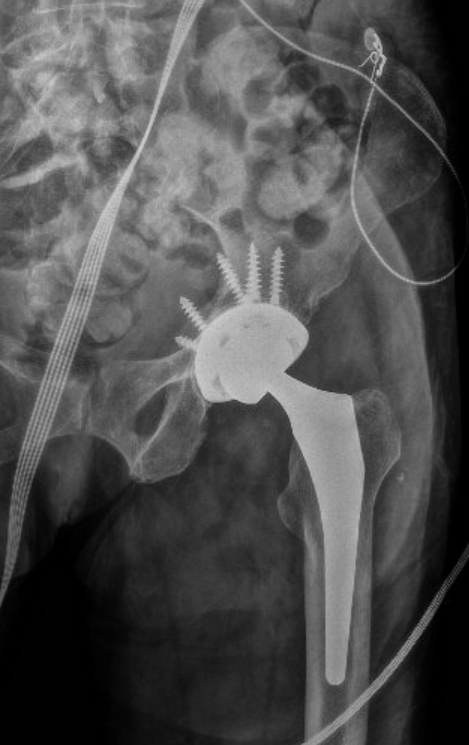
- Button batteries are distinguished on plain films most commonly by the “double ring sign” in AP view which is best shown in the lateral film above. Lateral views of a button battery may also show a step-off which is also evident in the AP x-ray.
- Management of a nasal button battery differs from many other foreign bodies due to the risk of rapid necrosis and septal perforation in as little as 7 hours.
- ED methods for removal of nasal foreign bodies include the “parent kiss” technique or bag valve mask to expel the foreign body, forcep or suction catheter removal, or use of a foley balloon.
- In this case, the object was ultimately removed by ENT with procedural sedation in the ED.
References:
Cohen JS, Agrawal D. Nose and Sinus Disorders in Infants and Children. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e.
McGraw Hill; 2020.Loh WS, Leong J, Tan HK: Hazardous foreign bodies: complications and management of button batteries in the nose. Ann Otol Rhinol Laryngol 112: 379, 2003. [PubMed: 12731636]