")


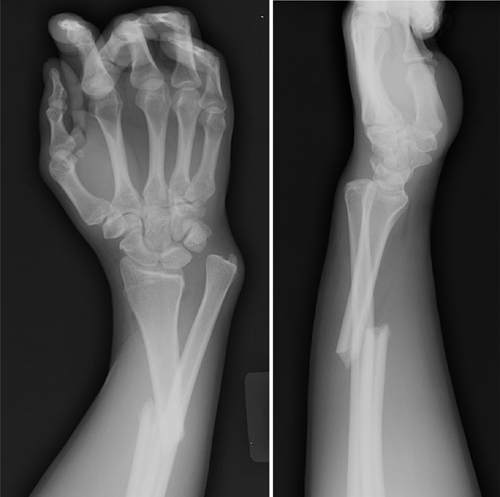
A 63 year old female is brought in by EMS after being found down. She has multiple ecchymoses on her chest and bilateral flanks. GCS is 6. After intubation, she is taken for CT head/cervical spine and a CT chest/abdomen/pelvis with contrast. Upon return from CT, x-rays are done (shown below) to further evaluate bruising and a laceration to her L elbow. What’s the diagnosis?
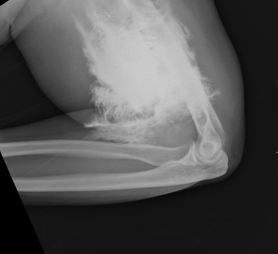
Answer: Contrast extravasation
- Predisposing factors for contrast extravasation
- Small IV gauge (22G or less)
- More distal access (hand)
- Rapid injection of contrast
- Incidence: up to 1% of patient receiving IV contrast through peripheral IV
- Most common symptoms: local pain, swelling
- Complications occur in < 1 % (more common with large volume and in patients with atherosclerosis, venous insufficiency, or impaired lymphatic drainage)
- Compartment syndrome
- Tissue necrosis
- Close monitoring required following extravasation
- Compartment checks, vascular checks, and monitoring of overlying skin
- Surgery consult for any signs of compartment syndrome or tissue injury
- Elevate limb, warm compresses may be used
- Patients rarely require more than conservative supportive treatment
References:
Sbitany, H., Koltz, P. F., Mays, C., Girotto, J. A., & Langstein, H. N. (2010). CT contrast extravasation in the upper extremity: Strategies for management. International Journal of Surgery, 8(5), 384-386. doi:10.1016/j.ijsu.2010.06.002
Sonis, J. D., et al (2018). Implications of iodinated contrast media extravasation in the emergency department. The American Journal of Emergency Medicine, 36(2), 294-296. doi:http://dx.doi.org/10.1016/j.ajem.2017.11.012